Greater Tuberosity Fractures
Learn about greater tuberosity fractures and treatment options
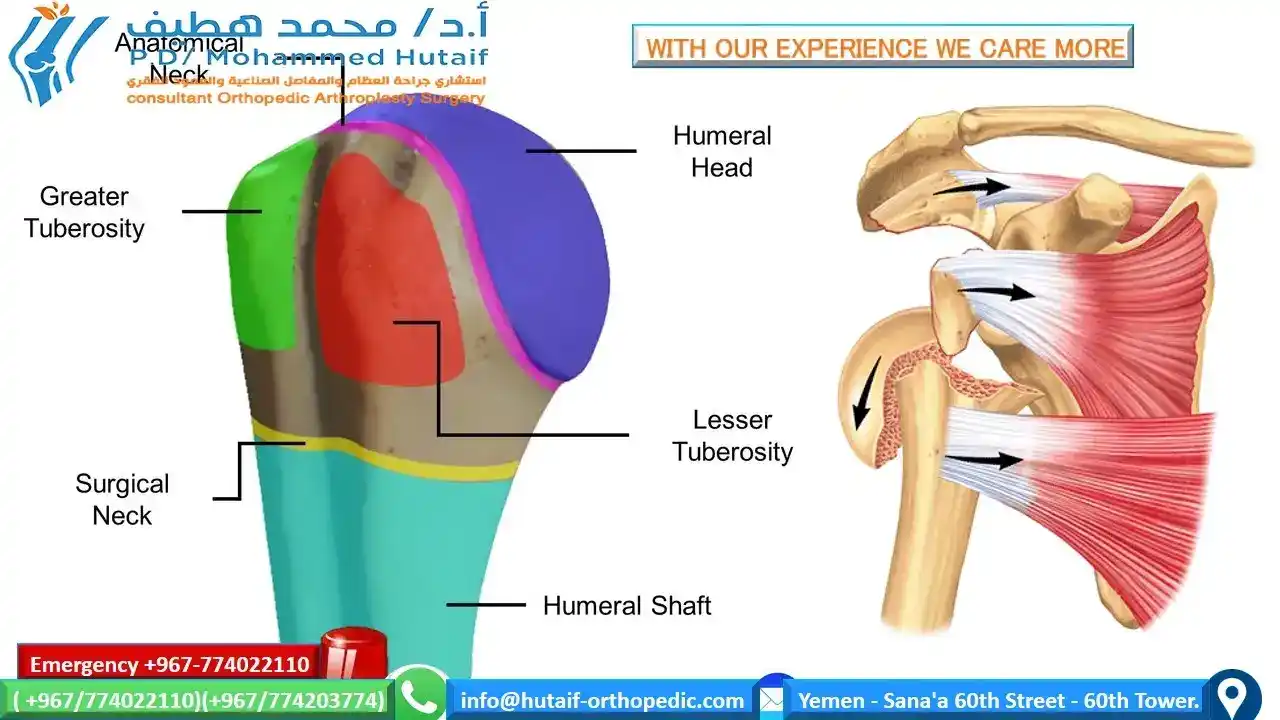
The greater tuberosity, located at the top of the humerus, connects with important rotator cuff muscles like the subspinal and supraspinatus muscles. It can fracture, either on its own or alongside other shoulder injuries such as a dislocated shoulder or complex humeral fracture. Displacement, where the bone is pushed out of its usual position, is possible.

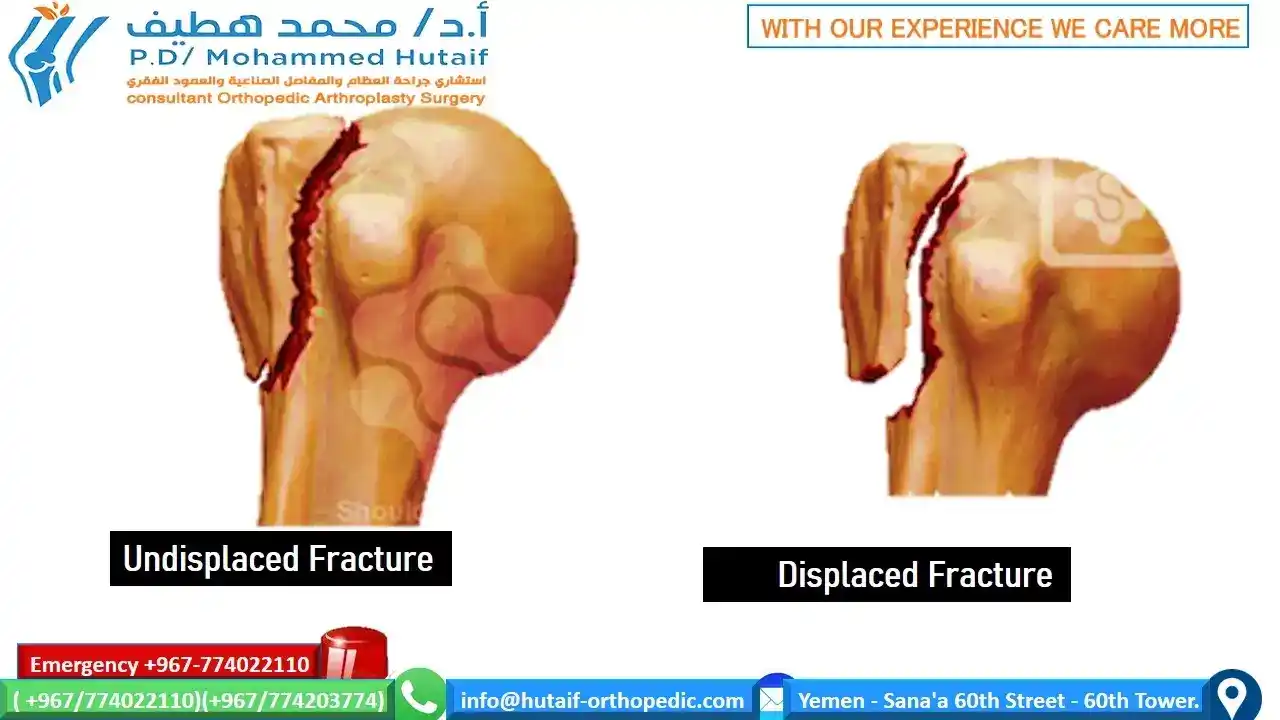
For non-displaced greater tuberosity fractures, non-surgical conservative treatment is an option.
Key indicators for non-surgical treatment are:
- Greater Tuberosity Fractures with less than 2 mm removed
Supporting indicators:
- Surgery risks outweigh benefits
Advantages of non-surgical treatment:
- No surgical or anesthesia risks
Disadvantages include:
- Potential risk of displacement
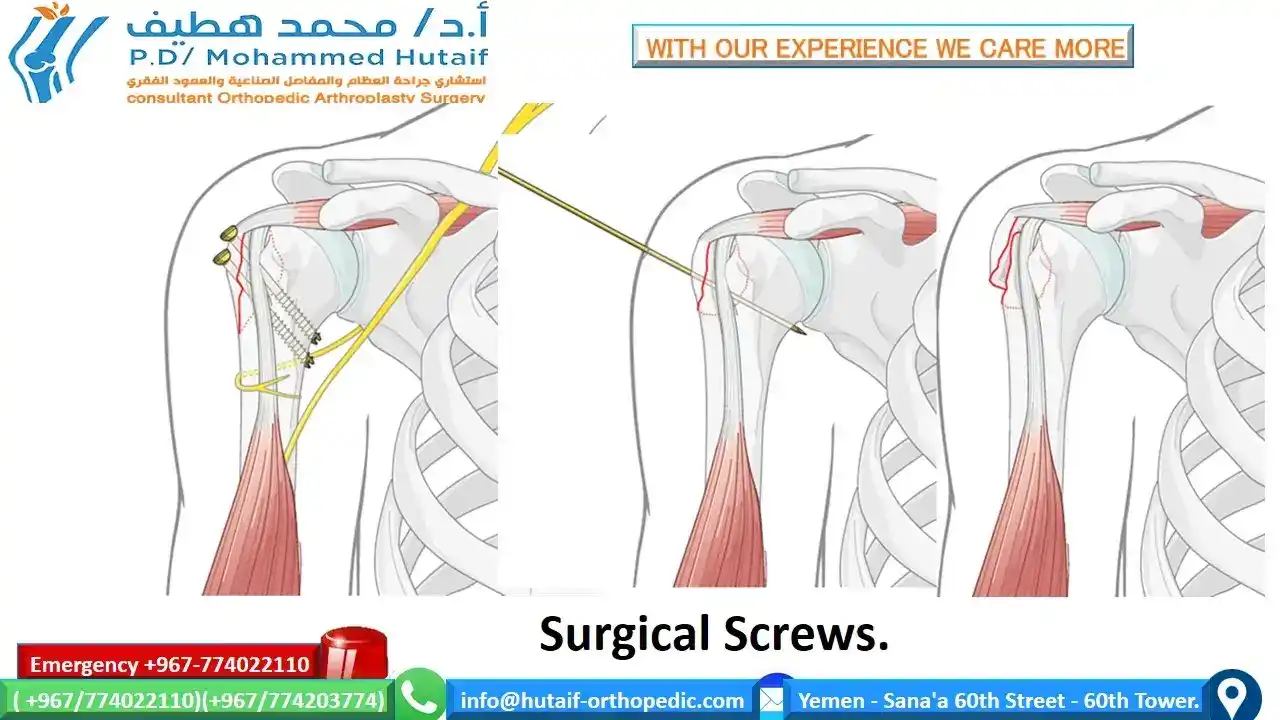
If there is a high risk of displacement or strong fixation is necessary for early movement, surgical treatment is an option. Advantages of surgery include reducing the risk of displacement and early mobilization. However, there may be a need to remove surgical devices as a disadvantage.
Undisplaced greater tuberosity fractures may not show up on an x-ray, leading to misdiagnosis as a shoulder sprain, deltoid injury, or rotator cuff injury. Shoulders that do not heal after a few weeks or suffer from stiffness and frozen shoulder may actually have an undisplaced fracture that can be seen on an MRI or ultrasound scan. Surgery is not necessary, but recovery can take a long time and frozen shoulder treatment may be required.
Displaced greater tuberosity fractures are rare, occurring in less than 2% of proximal humeral fractures, and are typically associated with anterior shoulder dislocations. As the greater tuberosity fragment detaches with its attached rotator cuff, it can develop impingement against the acromion and limit shoulder elevation and external rotation. Closed reduction is difficult, and surgery is typically necessary. This can involve a rotator cuff repair and acromioplasty, or a deltoid-splitting approach that removes the posterior acromion and avoids acromioplasty and weakening of the anterior deltoid. Fixation can be achieved through heavy sutures, wire, or screws. Large greater tuberosity fractures may require a deltopectoral approach for proper fixation.