
Shoulder osteoarthritis-Treatment
Shoulder osteoarthritis-Treatment
Nonsurgical Treatment
As with other arthritic conditions, initial treatment of arthritis of the shoulder is nonsurgical. Your doctor may recommend the following:
- Rest or change in activities. You may need to change the way you move your arm to avoid provoking pain.
- Physical therapy exercises may improve the range of motion in your shoulder.
- Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen, or naproxen, may reduce inflammation and pain. These medications can irritate the stomach lining and cause internal bleeding. They should be taken with food. Consult with your doctor before taking over-the-counter NSAIDs if you have a history of ulcers or are taking blood thinning medication.
- Corticosteroid injections in the shoulder can dramatically reduce the inflammation and pain. However, the effect is often temporary.
- Moist heat may provide temporary relief.
- Icing your shoulder for 20 to 30 minutes two or three times a day to reduce inflammation and ease pain.
- If you have rheumatoid arthritis, your doctor (typically a rheumatologist) may prescribe a disease-modifying drug, such as methotrexate.
- Dietary supplements, such as glucosamine and chondroitin sulfate may help relieve pain. (Note: There is little scientific evidence to support the use of glucosamine and chondroitin sulfate to treat arthritis. In addition, the U.S. Food and Drug Administration does not test dietary supplements. These compounds may cause negative interactions with other medications. Always consult your doctor before taking dietary supplements.)
Surgical Treatment
Your doctor may consider surgery if your pain causes disability and is not relieved with nonsurgical treatment.
Arthroscopy. Cases of mild glenohumeral arthritis may be treated with arthroscopy, During arthroscopy, the doctor inserts a small camera, called an arthroscope, into the shoulder joint. The camera displays pictures on a video monitor, and the doctor uses these images to guide miniature surgical instruments.
![Osteoarthritis of the shoulder is a gradual wearing of the articular cartilage that leads to pain and stiffness. As the joint surface degenerates, the subchondral bone remodels, losing its sphericity and congruity. The joint capsule also becomes thickened, leading to further loss of shoulder rotation. This painful condition is a growing problem in the aging population. In most cases, diagnosis of degenerative joint disease of the shoulder can be made with careful history, physical examination, and radiography. The symptoms and degree of shoulder arthritis visible on radiography determine the best treatment option. Mild degenerative joint disease can be treated with physical therapy and over-the-counter anti-inflammatory medications such as acetaminophen or nonsteroidal anti-inflammatory drugs. More advanced cases of osteoarthritis that are refractory to nonoperative management can be managed with corticosteroid injections. In severe cases, surgery is indicated. Surgical options include arthroscopic debridement, arthroscopic capsular release, and, in the most severe instances, hemiarthroplasty or total shoulder arthroplasty. Shoulder osteoarthritis, also known as degenerative joint disease of the shoulder, is a gradual, progressive, mechanical, and biochemical breakdown of the articular cartilage and other joint tissues, including bone and joint capsule. As the articular surface wears, friction within the joint increases, causing progressive loss of the normal load-bearing surfaces with pain and disability. There are many risk factors for shoulder osteoarthritis, including age, genetics, sex, weight, joint infection, history of shoulder dislocation, and previous injury. Certain occupations, such as heavy construction or overhead sports, are also risk factors. The prevalence of shoulder osteoarthritis is increasing as the population ages. Primary care physicians will be confronted with this disease at various levels of severity. This review highlights epidemiology, evaluation, current treatment options, and treatment results for osteoarthritis of the shoulder. SORT: KEY RECOMMENDATIONS FOR PRACTICE zoom_out_map Enlarge print Print Clinical recommendation Evidence rating References Axillary radiography should be performed because it provides the best images of joint-space narrowing to diagnose degenerative joint disease of the shoulder. This view also helps rule out dislocation. Anteroposterior radiography with the arm actively held at 45 degrees of abduction may reveal joint-space narrowing in patients with otherwise normal neutral anteroposterior radiography. C 10 The initial approach to early osteoarthritis should begin with activity modification, rest, and ice. Physical therapy, strength training, and aerobic exercise alleviate symptoms in certain cases; in other patients, over-the-counter medications may be sufficient for pain relief. C 12, 23, 24 Acetaminophen should be the first pharmacologic agent used to manage pain. Therapeutic effects are achieved at dosages of 3 to 4 g per day. C 13 The most common indications for shoulder arthroplasty are pain from shoulder arthritis with a loss of function that is unresponsive to conservative treatment; end-stage rotator cuff tear arthropathy; osteonecrosis; and a previously failed joint-sparing surgery or total shoulder arthroplasty. C 16 A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml. Epidemiology Musculoskeletal disorders have had a significant impact on the world's population. The current decade (2000–2010) has been named the “Bone and Joint Decade.”1 In the United States alone, musculoskeletal conditions account for 131 million patient visits per year, costing society about $215 billion.1 Arthritis and chronic joint symptoms affect one out of three adults, making it the most widespread disease in America.2 The prevalence of arthritis for all joints is higher in whites, men older than 45 years, women older than 55 years, overweight and inactive persons, and persons with less than eight years of education.2 Nearly 60 percent of those affected by osteoarthritis are older than 65 years, and the incidence is increasing.20 Osteoarthritis affects many joints throughout the body.3 Although not as common as other locations, shoulder osteoarthritis is just as debilitating. The loss of shoulder function can lead to depression, anxiety, activity limitations, and job-performance problems.4 The causes of shoulder osteoarthritis are divided into primary and secondary categories. Primary osteoarthritis has no specific cause, but is more prevalent and not isolated to older persons.5 Secondary osteoarthritis has a known cause or predisposing factor, such as major shoulder trauma, chronic dislocations, infection, congenital malformations, or chronic rotator cuff tear ( Table 16).5 TABLE 1 Classification of Degenerative Arthritis of the Glenohumeral Joint zoom_out_map Enlarge print Print Type Etiology Primary Unknown Secondary Atraumatic osteonecrosis Alcohol induced Corticosteroid therapy Cytotoxic drugs Gaucher's disease Lipid metabolism disorders Obesity Radiation Sickle cell disease Postinflammatory Crystal arthropathies Postinfection arthritis Rheumatoid arthritis Rotator cuff arthropathy Postsurgical Capsulorrhaphy arthropathy Intra-articular hardware (e.g., screws, staples) Overtightened anterior joint capsule (prior Putti-Platt repair) Posttraumatic Dislocation Malunion of the proximal humerus Posttraumatic avascular necrosis Subluxation Adapted with permission from Gerber A, Lehtinen JT, Warner JJ. Glenohumeral osteoarthritis in active patients: diagnostic tips and complete management options. Phys Sportsmed. 2003;4(31). http://www.physsportsmed.com/issues/2003/0403/gerber.htm. Accessed April 21, 2008. Evaluation The diagnosis of shoulder osteoarthritis involves a specific set of symptoms, physical examination findings, and changes to the bone, which are visible on radiography. The typical presenting symptom is progressive, activity-related pain that is deep in the joint and often localized posteriorly. As the disease progresses, night pain becomes more common. For many patients, the pain is present at rest and interferes with sleep. In advanced cases, the stiffness creates significant functional limitations. In younger patients, prior trauma, dislocation, or previous surgery for shoulder instability are factors associated with the development of osteoarthritis. Patients in the early stages of degenerative joint disease may complain of mild pain and may have unremarkable examinations. Radiography may show only subtle changes to the bone until there is more advanced destruction. The only objective evidence of the disease is articular cartilage wear, which may be shown on magnetic resonance imaging (MRI). In advanced cases, there is a loss of active and passive range of motion, in addition to pain. Physical examination will reveal painful crepitus, joint enlargement, and swelling. In severe cases, audible and palpable grinding may occur when a mechanical stress is placed on the shoulder. During the examination, it is important to exclude other shoulder pathologies that cause pain besides osteoarthritis (Table 2). Pain that is not induced by joint palpation or passive range of motion suggests bursitis, rotator cuff disease, or biceps tendinitis.7 Loss of passive and active range of motion may also occur with calcific tendinitis or idiopathic adhesive capsulitis. Radiography will show calcific tendinitis as radiodense calcium in the rotator cuff. In patients with adhesive capsulitis, shoulder joint radiography is typically normal. Morning stiffness may suggest rheumatoid arthritis. Intense inflammation, swelling, and erythema can be caused by gout, pseudo-gout, or a septic joint. A blood panel can help identify infection (i.e., white blood cell count greater than 11,000 per mm3 [11 × 109 per L] and white blood cell count in the joint fluid greater than 50,000 per mm3 [50 × 109 per L]). An erythrocyte sedimentation rate greater than 45 mm per hour may indicate rheumatoid arthritis, an underlying malignancy, or chronic infection. These blood tests are sensitive, but not specific in determining causes of shoulder pain.8 TABLE 2 Diagnosis of Shoulder Pathologies zoom_out_map Enlarge print Print Finding Probable diagnosis History Joint effusion Osteoarthritis Rheumatoid arthritis Septic arthritis Morning stiffness improved with activity Rheumatoid arthritis Night time shoulder pain Impingement Rotator cuff disease (partial or complete cuff tears) Pain or “clunking” sound with overhead motion Labral disorder Pain radiating down arm Disk disease (cervical) Stiffness worse with activity, improves with rest Osteoarthritis Physical examination Cervical range of motion decreased Disk disease (cervical) Crepitus Osteoarthritis Rheumatoid arthritis Decreased range of motion, specifically external rotation and abduction Osteoarthritis Soft tissue injury (frozen shoulder) Erythema, warmth Septic arthritis Rheumatoid arthritis Shoulder joint line tenderness Osteoarthritis Radiography Joint space narrowing (central, posterior, and superior erosion) Cufftear arthropathy Osteoarthritis Rheumatoid arthritis Marginal joint erosions Rheumatoid arthritis Normal joint Frozen shoulder Septic arthritis Osteophytes Osteoarthritis Subchondral sclerosis Osteoarthritis Imaging studies are essential to diagnosing degenerative joint disease. In most cases, conventional radiography demonstrates shoulder osteoarthritis9 (Table 2). Early in the disease process, radiographic evidence of degenerative joint disease may include joint-space narrowing (mild), osteophytes (small), subchondral sclerosis, cysts, and eburnation or advanced articular cartilage loss (Figure 1). The axillary view provides the best image to look for joint-space narrowing and helps rule out dislocations. Anteroposterior radiography, with the arm held at 45 degrees of abduction, may also show early joint-space narrowing.10 Computed tomography arthrograms can localize articular defects, whereas MRI reveals soft-tissue pathologies and subtle changes in articular cartilage. Subchondral edema visible on MRI suggests advanced articular cartilage involvement.11 FIGURE 1. zoom_out_map Enlarge print Print Preoperative anteroposterior radiograph illustrating degenerative changes. Current Treatment Options MEDICAL MANAGEMENT Presently, there are no known interventions that alter the natural history of early osteoarthritis; therefore, the main objectives in treatment are to control pain and restore function. The initial approach to osteoarthritis treatment begins with activity modification, rest, and ice. Physical therapy, strength training, and aerobic exercise help alleviate symptoms.12 Acetaminophen should be the first pharmacologic agent used to manage pain, with therapeutic effects achieved at dosages of 3 to 4 g per day.13 Nutritional supplements, such as glucosamine and chondroitin, are pharmacologic alternatives to acetaminophen, although only anecdotal evidence supports their use for shoulder osteoarthritis. The mainstay of pharmacotherapy for degenerative joint disease has been the nonselective and selective cyclooxygenase-2 (COX-2) inhibitors, or nonsteroidal anti-inflammatory drugs (NSAIDs) (Table 314). Nonselective COX-2 inhibitors (e.g., ibuprofen [Motrin], diclofenac [Voltaren], naproxen [Naprosyn]) and selective COX-2 inhibitors (e.g., celecoxib [Celebrex]) have been effective in alleviating osteoarthritis symptoms, but have varying side effects. Side effects can include gastrointestinal irritation, stomach ulcerations, bleeding, or renal failure from long-term use. In advanced osteoarthritis cases with inflammation, an injection of a corticosteroid, such as triamcinolone acetonide (Kenalog; 1 to 2 mL of 40 mg per mL) with lidocaine 1% (Xylocaine), into the affected joint can help relieve pain and swelling. TABLE 3 Guide to NSAID Therapy zoom_out_map Enlarge print Print Cardiovascular risk level No or low NSAID gastrointestinal risk NSAID gastrointestinal risk No cardiovascular risk (no aspirin) Traditional NSAID Consider non-NSAID therapy Traditional NSAID plus PPI or COX-2 inhibitor plus PPI* (if necessary) Cardiovascular risk (consider aspirin) Consider non-NSAID therapy Consider non-NSAID therapy Traditional NSAID† plus PPI if gastrointestinal risk warrants gastroprotection A gastroprotective agent must be added if a traditional NSAID† is prescribed COX-2 = cyclooxygenase-2; NSAIDs = nonsteroidal anti-inflammatory drugs; PPI = proton pump inhibitor. *—The U.S. Food and Drug Administration has determined that over-the-counter and prescription NSAIDs (including selective COX-2 agents), when used as monotherapy, may be linked to potentially life-threatening gastrointestinal bleeding. †—NSAIDS should be used cautiously in patients taking aspirin. Adapted with permission from Fendrick AM. COX-2 inhibitor use after Vioxx: careful balance or end of the rope? [editorial]. Am J Manag Care. 2004;10(11):741. SURGICAL MANAGEMENT If conservative therapies fail, there are many surgical options available. Joint preservation surgery is preferable for patients younger than 55 to 60 years or those with early stage degenerative joint disease of the shoulder. The operative procedure should match the patient's symptoms or functional limitations. Arthroscopic debridement, capsular release, corrective osteotomies, and interposition arthroplasty are surgical options that attempt to reduce symptoms while preserving the native joint.15 Arthroscopic debridement with capsular release is the most common surgical treatment. It is most effective in patients younger than 55 to 60 years with moderate pain and significant passive motion restrictions. Debridement removes mechanical irritants, unstable cartilage flaps, or loose bodies. Inflamed synovium can be treated via synovectomy, and the stiff contracted joint capsule can be released to restore passive joint mobility and unload articular surfaces. Arthrodesis (shoulder fusion) is an option for patients younger than 45 to 50 years with severe arthritis or for those who are not suitable candidates for total shoulder replacement. This procedure eliminates pain by fusing the humeral head to the glenoid, thus eliminating painful motion interface. Shoulder arthroplasty is recommended for patients with severe shoulder osteoarthritis. The most common indications for shoulder arthroplasty are pain from shoulder arthritis with a loss of function that is unresponsive to conservative treatment; end-stage rotator cuff tear arthropathy; osteonecrosis; and a previously failed joint-sparing surgery or total shoulder arthroplasty.16 Most recent studies support the use of a total shoulder arthroplasty, which involves replacing the glenoid and humerus 17,18 (Figure 2). In certain instances, a hemiarthroplasty (humerus only) may be an acceptable option. Major contraindications to shoulder replacement are: active or recent infection, neuropathic joint, complete paralysis of deltoid or rotator cuff muscles, debilitating medical status, or uncorrectable shoulder instability. FIGURE 2. zoom_out_map Enlarge print Print Postoperative radiograph following total shoulder arthroplasty. Shoulder arthroplasty is typically done under general anesthesia. A regional nerve anesthetic (interscalene block) can supplement general anesthesia and provide perioperative pain control. After careful surgical exposure, the glenoid fossa is resurfaced with a solid polyethylene component, and the humeral head is resected along the anatomic neck and replaced with a metal prosthesis. Newer prostheses, called reverse or inverse shoulder replacements, have been designed specifically for use in rotator-cuff–deficient shoulders. The procedure lasts one to three hours, followed by a two- to four-day postoperative hospitalization. Blood loss is minimal, and patients who start with a preoperative hemoglobin above 11 g per dL (110 g per L) should not need transfusions. Donating blood before surgery is not recommended.19 Pain is controlled in the hospital with opioids via intravenous patient-controlled analgesia. A sling should be used for three to six weeks to protect the repair. Patients usually require some assistance with normal daily activities for approximately four to six weeks after surgery. Postoperative rehabilitation begins immediately with joint motion, in-home exercises, and a therapist-supervised program (Table 4).20 The initial six weeks of rehabilitation focus on stretching exercises to optimize the flexibility of the joint. When flexibility and range-of-motion goals have been achieved (usually at six to eight weeks), the strengthening can begin. Normal activities of daily living can be resumed within six weeks of surgery, and patients can often return to athletic activities within four months. After shoulder arthroplasty, patients can expect alleviation of pain and a significant improvement in range of motion.18 Improvement in function may continue up to two years after surgery.21 TABLE 4 Postoperative Rehabilitation Sequencing zoom_out_map Enlarge print Print Exercise Postoperative day Active hand, forearm, elbow motion 1 Passive shoulder motion 1 Pulley 21 Wand or cane 35 Isometrics 35 Information from reference 20. Treatment Results NONSURGICAL TREATMENT Nonsurgical osteoarthritis treatments can temporize symptoms; however, they do not alter natural history and have had unsatisfactory results. Nonpharmacologic measures, such as aerobic exercise and strengthening, are unproven in the shoulder.22 One study has shown that acetaminophen was more effective than placebo at pain reduction, but less effective than NSAIDs.23 NSAIDs were also associated with more frequent gastrointestinal events than acetaminophen.23 Two randomized placebo-controlled studies have been published since 2003. One found no significant difference between placebo and acetaminophen, and the other found acetaminophen to be more effective than placebo, and celecoxib to be more effective than acetaminophen.13,24 Pharmacologic results show that newer COX-2 selective inhibitors are not more effective than nonselective NSAIDs for treating knee and hip osteoarthritis.25,26 However, the Celecoxib Long Term Arthritis Safety Study (CLASS) illustrated that the COX-2 inhibitor celecoxib was associated with significantly less gastrointestinal events than traditional NSAIDs.27 In recent years, studies have shown certain COX-2 inhibitors to be associated with an increased cardiovascular risk, resulting in the removal of rofecoxib (Vioxx) from the market. Additional data suggest that the nonselective NSAIDs may also cause an increase in adverse cardiovascular events.28,29 More studies are needed to demonstrate effectiveness and serious cardiovascular side effects of NSAIDs and COX-2 selective inhibitors. Nutritional supplements are widely used for osteoarthritis treatment, although the U.S. Food and Drug Administration has not approved them for this use. The most common supplements are glucosamine and chondroitin. Glucosamine has been shown to provide moderate symptomatic relief over placebo, but the overall effectiveness of these supplements remains uncertain.30 At this time, there is a paucity of evidence to support the use of these supplements in shoulder degenerative joint disease. SURGICAL TREATMENT Few studies exist on joint-preservation surgery for the shoulder. There are several case reports and small series that present cartilage resurfacing procedures for young patients with focal chondral defects.31,32 The largest series on arthroscopic treatment consists of 25 patients with early to moderate osteoarthritis, treated with lavage, partial synovectomy, and subacromial decompression.15 The mean follow-up was 34 months, and the authors demonstrated good or excellent outcomes in 80 percent of patients. The authors concluded that arthroscopic debridement was reasonable for early shoulder osteoarthritis treatment. Surgical prerequisites included concentric humeral head and glenoid with visible joint space on axillary radiography. Prosthetic total shoulder arthroplasty is the treatment of choice for severe degenerative joint disease. Studies show that total shoulder arthroplasty provides excellent clinical results with good durability. The results of total shoulder arthroplasty have been shown to be superior to hemiarthroplasty, in which only the humerus is resurfaced.33 As early as 1982, one study reported that 90 percent of patients who underwent total shoulder arthroplasty had satisfactory results at minimum two-year follow-up.34 As of 1988, only two of the 615 patients who had undergone total shoulder arthroplasty required further surgery. Another paper with 12-year mean follow-up demonstrated satisfactory pain relief in 83 percent of shoulders, with an average improvement of 40-degree active abduction, and yielding an overall average range of motion of 117 degrees.18 Despite concerns about glenoid loosening, long-term studies have shown high rates of survivorship. Another study of patients younger than 50 years, with minimum five-year and mean 12-year follow-up, found a prosthesis survival rate of 97 percent at five years, 97 percent at 10 years, and 84 percent at 15 years.16 This study illustrates that total shoulder arthroplasty improves functional range of motion with good long-term pain relief. The average orthopedic surgeon performs only two total shoulder arthroplasties per year, and recent data has shown that surgeon and hospital volume significantly influence surgical outcomes.32,35 Surgeons with higher volumes of arthroplasties have better patient outcomes and fewer complications. When total shoulder arthroplasty is performed under appropriate clinical indication, complete pain relief and normal or near-normal restoration of function is often the result. Experts predict that surgical outcomes following total shoulder arthroplasty will continue to improve with newer implant designs and fixation methods. expand_moreAuthor Information PETER J. MILLETT, MD, MSc, is the director of shoulder surgery at the Steadman Hawkins Clinic in Vail, Colo. He received his medical degree from Dartmouth Medical School, Hanover, N.H., and his master of science degree from University of Cambridge, Cambridge, England. Dr. Millett completed an orthopaedic surgery residency at Hospital for Special Surgery, Weill Medical College of Cornell University (formerly Cornell University Medical College), New York, N](https://hutaif-orthopedic.com/upload/1658863530.webp)
shoulder Arthroscopy
Because the arthroscope and surgical instruments are thin, the surgeon can use very small incisions rather than the larger incision needed for standard, open surgery.
During the procedure, your doctor can debride (clean out) the inside of the joint. Although the procedure provides pain relief, it will not eliminate the arthritis from the joint. If the arthritis progresses, further surgery may be needed in the future.
Shoulder joint replacement (arthroplasty). Advanced arthritis of the glenohumeral joint can be treated with shoulder replacement surgery. In this procedure, damaged parts of the shoulder are removed and replaced with artificial components, called a prosthesis.
Replacement surgery options include:
Hemiarthroplasty. Just the head of the humerus is replaced by an artificial component.
Total shoulder arthroplasty. Both the head of the humerus and the glenoid are replaced. A plastic cup is fitted into the glenoid, and a metal ball is attached to the top of the humerus.
Reverse total shoulder arthroplasty. In a reverse total shoulder replacement, the socket and metal ball are opposite a conventional total shoulder arthroplasty. The metal ball is fixed to the glenoid, and the plastic cup is fixed to the upper end of the humerus. A reverse total shoulder replacement works better for people with cuff tear arthropathy because it relies on different muscles — not the rotator cuff — to move the arm.
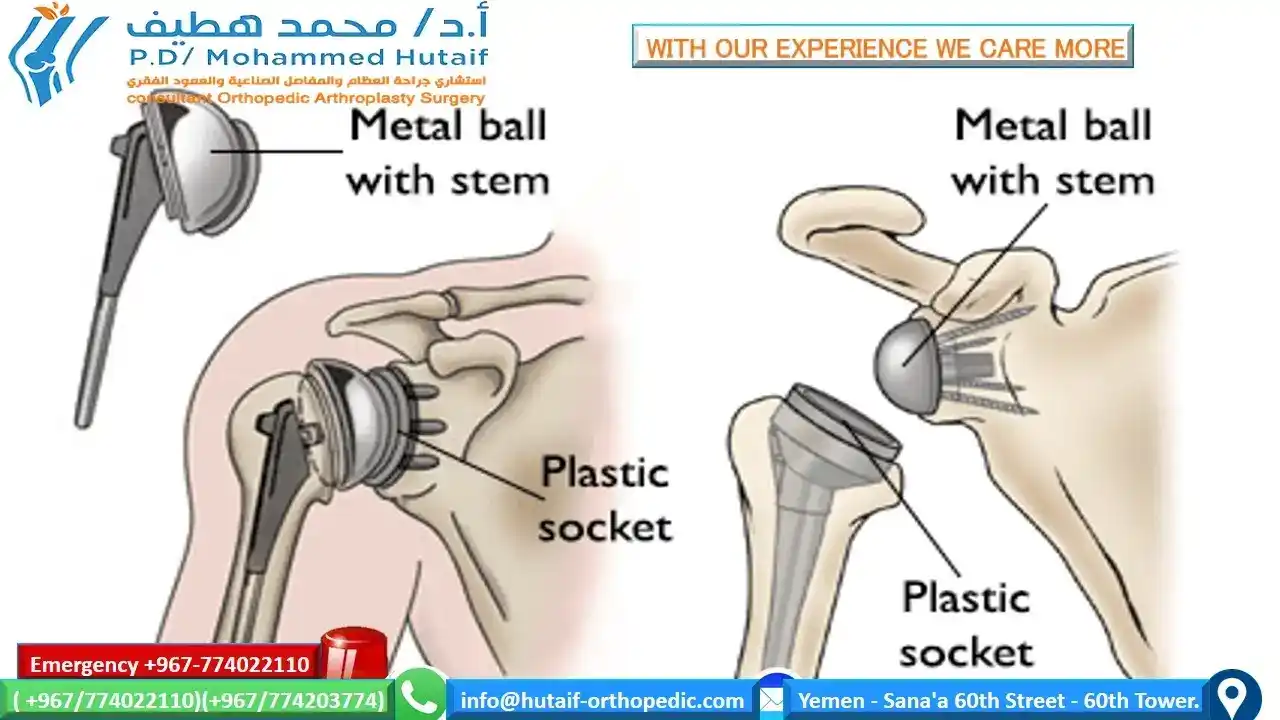
(Left) A conventional total shoulder replacement (arthroplasty) mimics the normal anatomy of the shoulder. (Right) In a reverse total shoulder replacement, the plastic cup inserts on the humerus, and the metal ball screws into the shoulder socket.
Resection arthroplasty. The most common surgical procedure used to treat arthritis of the acromioclavicular joint is a resection arthroplasty. Depending on your specific situation, this procedure may be performed either arthroscopically or through traditional open surgery
In this procedure, the doctor removes a small amount of bone from the end of the collarbone, leaving a space that gradually fills in with scar tissue.
Recovery. Surgical treatment of arthritis of the shoulder is generally very effective in reducing pain and restoring motion. Recovery time and rehabilitation plans depend upon the type of surgery performed.
Pain management. After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor and to stop taking them as soon as your pain begins to improve. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Complications. As with all surgeries, there are some risks and possible complications. Potential problems after shoulder surgery include infection, excessive bleeding, blood clots, and damage to blood vessels or nerves.
Your doctor will discuss the possible complications with you before your operation
In This Article:
To assist doctors in the management of glenohumeral joint osteoarthritis, the American Academy of Orthopaedic Surgeons has conducted research to provide some useful guidelines. These are recommendations only and may not apply to every case. For more information: Glenohumeral Joint Osteoarthritis - Clinical Practice Guideline (CPG) | American Academy of Orthopaedic Surgeons (aaos.org)