Orthopedic MD Oral Examination: Diagnosis and Management of Humeral Shaft Fractures
Diagnosis and Management for Humeral Shaft Fractures

Interpretation of X-ray Image
The X-ray image reveals a displaced fracture located in the middle third of the left humerus. There are no signs of dislocation in the left shoulder. On examination, the patient presented with pain and deformity in the left middle humerus, with no pain at the shoulder or elbow joints. Based on these findings, the fracture can be classified as a mid-shaft humerus fracture.
Click here to see more
Humeral Shaft Fractures
SUMMARY
Humeral shaft fractures are common fractures of the diaphysis of the humerus, which may be associated with radial nerve injury. Diagnosis is made with orthogonal radiographs of the humerus. Treatment can be nonoperative or operative depending on location of fracture, fracture morphology, and association with other ipsilateral injuries.
EPIDEMIOLOGY
- Incidence: 3-5% of all fractures
- Demographics:
- Bimodal age distribution
- Young patients with high-energy trauma
- Elderly, osteopenic patients with low-energy injuries
ANATOMY
Osteology
- Humeral shaft is cylindrical
- Distally humerus becomes triangular
- Intramedullary canal terminates 2 to 3 cm proximal to the olecranon fossa
Muscles
- Insertion for:
- Pectoralis major
- Deltoid
- Coracobrachialis
- Origin for:
- Brachialis
- Triceps
- Brachioradialis
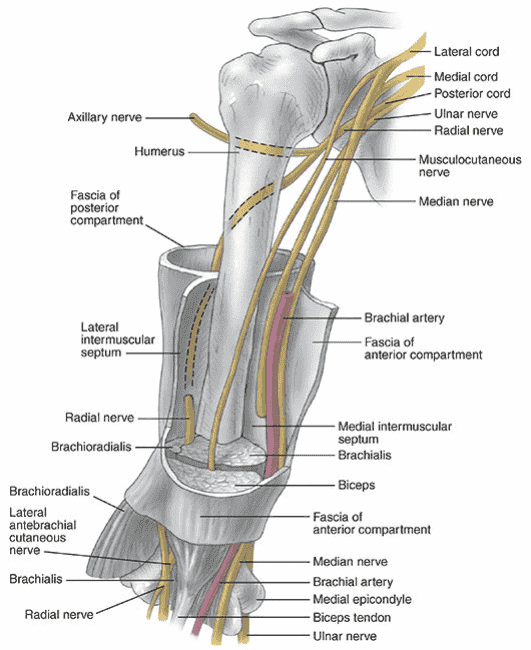
Nerve
- Radial nerve
- Courses along spiral groove
- 14cm proximal to the lateral epicondyle
- 20cm proximal to the medial epicondyle
CLASSIFICATION
OTA
| Bone Number | Fracture Location | Fracture Pattern |
|---|---|---|
| 1 | 2 | Simple:A, Wedge:B, Complex:C |
Descriptive
- Fracture location: proximal, middle or distal third
- Fracture pattern: spiral, transverse, comminuted
- Holstein-Lewis fracture: a spiral fracture of the distal one-third of the humeral shaft commonly associated with neuropraxia of the radial nerve (22% incidence)
PRESENTATION
Symptoms
- Pain
- Extremity weakness
Physical exam
- Examine overall limb alignment
- Will often present with shortening and in varus
- Preoperative or pre-reduction neurovascular exam is critical
- Examine and document status of radial nerve pre and post-reduction
IMAGING
Radiographs
- Views: AP and lateral
- Be sure to include joint above and below the site of injury
- Transthoracic lateral may give better appreciation of sagittal plane deformity; rotating the patient prevents rotation of the distal fragment avoiding further nerve or soft tissue injury
- Traction views may be necessary for fractures with significant shortening, proximal or distal extension but not routinely indicated
TREATMENT
Nonoperative
Coaptation splint followed by functional brace
- Indications:
- Indicated in vast majority of humeral shaft fractures
- Criteria for acceptable alignment include:
- < 20° anterior angulation
- < 30° varus/valgus angulation
- < 3 cm shortening
- Absolute contraindications:
- Severe soft tissue injury or bone loss
- Vascular injury requiring repair
- Brachial plexus injury
- Relative contraindications:
- See relative operative indications section
- Radial nerve palsy is NOT a contraindication to functional bracing
- Outcomes: 90% union rate; increased risk with proximal third oblique or spiral fracture; varus angulation is common but rarely has functional or cosmetic sequelae
- DCO: closed humerus fractures, including low velocity GSW, should be initially managed with a splint or sling; type of fixation after trauma should be directed by acceptable fracture alignment parameters, fracture pattern and associated injuries
Operative
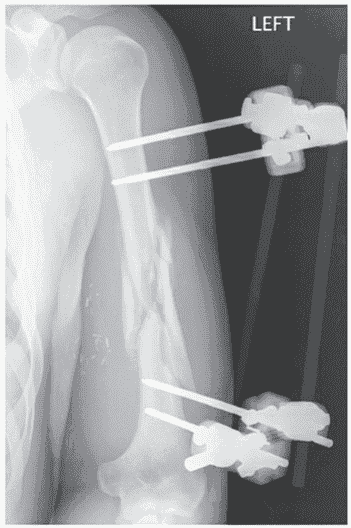
- External fixation
- Indications:
- High energy complex or comminuted fracture
- Open fracture
- Significant soft tissue or bony defect
- Floating elbow
- Hemodynamically unstable polytrauma
- Concomitant vascular injury
- Indications:
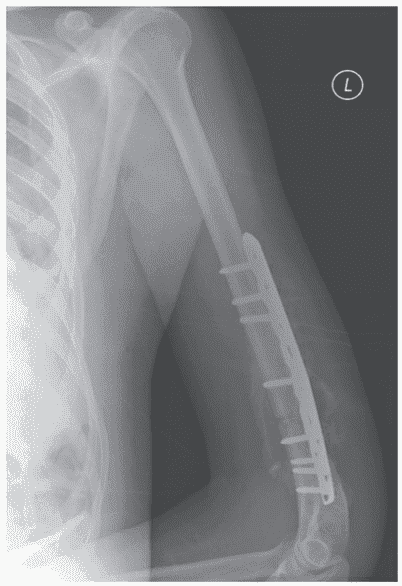
- Open reduction and internal fixation (ORIF)
- Absolute indications:
- Open fracture
- Vascular injury requiring repair
- Brachial plexus injury
- Ipsilateral forearm fracture (floating elbow)
- Compartment syndrome
- Periprosthetic humeral shaft fractures at the tip of the stem
- Relative indications:
- Bilateral humerus fracture
- Polytrauma or associated lower extremity fracture
- Pathologic fractures
- Fracture characteristics
- Distraction at fracture site
- Short oblique or transverse fracture pattern
- Intraarticular extension
- Absolute indications:
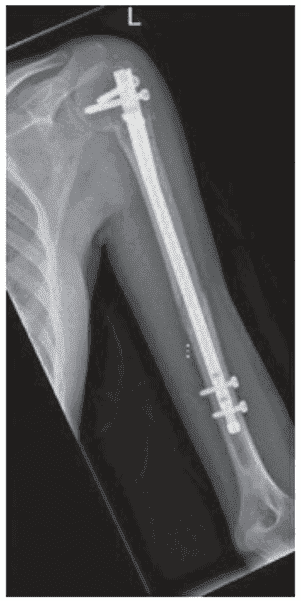
- Intramedullary Nailing (IMN)
- Relative indications:
- Pathologic fractures
- Segmental fractures
- Severe osteoporotic bone
- Overlying skin compromise limits open approach
- Polytrauma
- Relative indications:
COMPLICATIONS
- Humeral shaft fx nonunion: no callous on radiograph and gross motion at the fracture site at 6 weeks from injury has a 90-100% PPV of going on to nonunion in closed humeral shaft fractures
- Malunion: varus angulation is common but rarely has functional or cosmetic sequelae; risk factors: transverse fracture patterns, radial nerve palsy
- Radial nerve palsy: incidence seen in 8-15% of closed fractures; increased incidence distal one-third fractures (22%); iatrogenic radial nerve palsy is most common following ORIF via a lateral approach (20%) or posterior approach (11%)
Click here to see more
Humeral Shaft Fractures
EPIDEMIOLOGY
- Common injury, representing 3% to 5% of all fractures
- Incidence is 14.5 per 100,000 per year.
- Two percent to 10% are open fractures.
- Sixty percent involve middle third, 30% involve proximal third, and 10% involve distal third of the diaphysis.
- Bimodal age distribution with a peak in third decade in men and seventh/eighth decade in women
ANATOMY
Humeral shaft extends from the pectoralis major insertion to the supracondylar ridge. Cross-sectional shape of humeral shaft changes from cylindric proximally to a narrower triangular shape distally. Vascular supply to the humeral diaphysis arises from perforating branches of the brachial artery, with the main nutrient artery entering the medial humerus distal to the midshaft.

MECHANISM OF INJURY
- Direct (most common): Direct trauma to the arm from a blow or motor vehicle accident results in a transverse or comminuted fracture.
- Indirect: A fall on an outstretched arm results in transverse or oblique fractures, especially in the elderly. Throwing injuries with extreme muscular contraction and arm wrestling with rotational forces have also been reported to cause spiral humeral shaft fractures.
- Fracture pattern depends on the type of force applied:
- Compressive: proximal or distal humerus fractures
- Bending: transverse fractures of the humeral shaft
- Torsional: spiral fractures of the humeral shaft
- Torsional and bending: oblique fracture, often accompanied by a butterfly fragment
CLINICAL EVALUATION
- Patients with humeral shaft fractures typically present with pain, swelling, deformity, and shortening of the affected arm.
- A careful neurovascular examination is essential, with particular attention to radial nerve function. In cases of extreme swelling, serial neurovascular examinations are indicated with possible measurement of compartment pressures.
- Physical examination frequently reveals gross motion with crepitus on gentle manipulation.
- Soft tissue abrasions and minor lacerations must be differentiated from open fractures.
- Intra-articular extension of open fractures may be determined by intra-articular injection of saline distant from the wound site and noting extravasation of fluid from the wound.
RADIOGRAPHIC EVALUATION
- Anteroposterior (AP) and lateral radiographs of the humerus should be obtained, including the shoulder and elbow joints. To obtain views at 90 degrees from each other, the patient, NOT the arm, should be rotated (transthoracic lateral) because manipulation of the injured extremity will typically result in distal fragment rotation only.
- Traction radiographs may aid in fracture definition in cases of severely displaced or comminuted fractures. Computed tomography, bone scans, and magnetic resonance imaging (MRI) are rarely indicated except in cases in which pathologic fracture is suspected.
CLASSIFICATION
Descriptive
| Classification Criteria | Subcategories |
|---|---|
| Open versus closed | |
| Location | Proximal third, middle third, distal third |
| Displacement | Nondisplaced, displaced |
| Direction and character | Transverse, oblique, spiral, segmental, comminuted |
| Intrinsic condition of bone | Normal, osteopenic, pathologic |
| Articular extension |
Orthopaedic Trauma Association Classification
See Fracture and Dislocation Compendium at ota.org.
TREATMENT
Goals are fracture union with acceptable humeral alignment and patient return to preinjury level of function. Both patient and fracture characteristics, including patient age and functional level, presence of associated injuries, soft tissue status, and fracture pattern, need to be considered when selecting an appropriate treatment option.
NONOPERATIVE
Most humeral shaft fractures (>90%) will heal with nonsurgical management. Nonoperative treatment requirements include:
- An understanding by the treating physician of the postural and muscular forces to be controlled
- Close patient supervision and follow-up
- A cooperative and preferably upright and mobile patient
- An acceptable fracture reduction
- Intact/innervated arm musculature (e.g., intact brachial plexus)
Historically, 10 degrees of anterior (sagittal) angulation, 25 degrees of varus or 10 degrees of valgus (coronal) angulation, and up to 3 cm of bayonet apposition are acceptable and will not compromise function or appearance. Even angulation beyond these parameters has never been shown to affect function, only cosmesis.
- Hanging cast:
- Uses dependency traction by the weight of the cast and arm to effect fracture reduction.
- Indications include displaced midshaft humeral fractures with shortening, particularly spiral or oblique patterns. Transverse or short oblique fractures represent relative contraindications because of the potential for distraction and healing complications.
- Rarely used because the patient must remain upright or semiupright at all times with the cast in a dependent position for effectiveness.
- May be exchanged for functional bracing following early callus formation.
- More than 95% union is reported.
- Coaptation splint:
- Uses dependency traction and hydrostatic pressure to effect fracture reduction but with greater stabilization and less distraction than a hanging arm cast. The forearm is suspended in a collar and cuff.
- Indicated for the acute treatment of humeral shaft fractures with minimal shortening and for short oblique or transverse fracture patterns that may displace with a hanging arm cast
- Disadvantages include irritation of the patient’s axilla and the potential for splint slippage.
- May be exchanged for functional bracing 1 to 2 weeks after injury.
- Thoracobrachial immobilization (Velpeau dressing):
- Used only in elderly patients or children who are unable to tolerate other methods of treatment and in whom comfort is the primary concern.
- Indicated for minimally displaced or nondisplaced fractures that do not require reduction.
- Passive shoulder pendulum exercises may be performed within 1 to 2 weeks after injury.
- May be exchanged for functional bracing 1 to 2 weeks after injury.
- Functional bracing:
- Uses hydrostatic soft tissue compression to effect and maintain fracture alignment while allowing motion of adjacent joints.
- Typically applied 1 to 2 weeks after injury, after the patient has been placed in a hanging arm cast or coaptation splint, and pain/swelling has subsided.
- Consists of an anterior and posterior (or medial–lateral) shell held together with Velcro straps (Fig. 16.2)
- Success depends on an upright patient and brace tightening daily as well as functioning upper arm musculature.
- Contraindications include massive soft tissue injury, an unreliable patient, and an inability to obtain or maintain acceptable fracture reduction.
- A collar and cuff may be used to support the forearm, but sling application may result in varus angulation.
- The functional brace is worn for a minimum of 8 weeks after fracture or until radiographic evidence of union.
OPERATIVE
Indications for operative treatment include:
- Multiple trauma
- Inadequate closed reduction or unacceptable malunion
- Pathologic fracture
- Associated vascular injury
- “Floating elbow”
- Segmental fracture
- Intra-articular fracture extension
- Bilateral humeral fractures
- Open fracture
- Neurologic loss following penetrating trauma
- Brachial plexus injury
- Radial nerve palsy after fracture manipulation (controversial)
- Nonunion
- Unfavorable body habitus such as morbid obesity or pendulous breasts (relative indication)
- Chronic shoulder or elbow stiffness as it results in increased motion through the fracture and increases the risk on nonunion (relative indication)
Surgical approaches to the humeral shaft include:
- Anterolateral approach: preferred for proximal third humeral shaft fractures; radial nerve identified in the interval between the brachialis and brachioradialis and traced proximally. The brachialis muscle is split to afford access to the shaft. This can be extended proximally to the shoulder.
- Anterior approach: muscular interval between the biceps and brachialis muscles
- Posterior approach: provides excellent exposure to most of the humerus, including the elbow, but cannot be extended proximally to the shoulder; muscular interval is between the lateral and long heads of the triceps. The medial head is split. The radial nerve must be identified in the spiral groove usually at the midportion of the arm.
Postoperative Rehabilitation:
Range-of-motion exercises for the hand and wrist should be started immediately after surgery; shoulder and elbow range of motion should be instituted as pain subsides.
COMPLICATIONS
- Radial nerve injury occurs in up to 22% of cases.
- Vascular injury: uncommon but may be associated with fractures of the humeral shaft lacerating or impaling the brachial artery or with penetrating trauma. The brachial artery has the greatest risk for injury in the proximal and distal third of arm. It constitutes an orthopaedic emergency; arterial inflow should be established within 6 hours. At surgery, the vessel should be explored and repaired and the fracture stabilized.
- Nonunion: occurs in up to 15% of cases.
- Malunion: may be functionally inconsequential; arm musculature and shoulder, elbow, and trunk range of motion can compensate for angular, rotational, and shortening deformities.
IMAGES