Understanding proximal humerus fractures in children: causes, symptoms, and treatment
Learn about the causes, symptoms, and treatment options for proximal humerus fractures in children of different ages. Find out about the complications, prognosis, and acceptable levels of deformity associated with these fractures.
PROXIMAL HUMERUS FRACTURES
PEDIATRIC SHOULDER
Epidemiology
These account for <5% of fractures in children.
Incidence ranges from 1.2 to 4.4 per 10,000 per year.
They are most common in adolescents owing to increased sports participation and are often metaphyseal, physeal, or both.
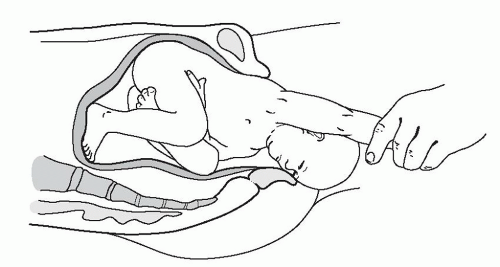
Neonates may sustain birth trauma to the proximal humeral physis, representing 1.9% to 6.7% of physeal injuries (Fig. 43.1).
Anatomy
Eighty percent of humeral growth occurs at the proximal physis, giving this region great remodeling potential.
There are three centers of ossification in the proximal humerus:
- Humeral head: This ossifies at 6 months.
- Greater tuberosity: This ossifies at 1 to 3 years.
- Lesser tuberosity: This ossifies at 4 to 5 years.
The greater and lesser tuberosities coalesce at 6 to 7 years and then fuse with the humeral head between 7 and 13 years of age.
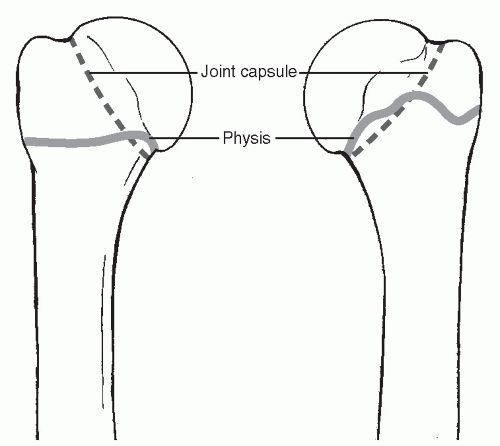
The joint capsule extends to the metaphysis, rendering some fractures of the metaphysis intracapsular (Fig. 43.2).
The primary vascular supply is via the anterolateral ascending branch of the anterior circumflex artery, with a small portion of the greater tuberosity and inferior humeral head supplied by branches of the posterior circumflex artery.
The physis closes at ages 14 to 17 years in girls and at ages 16 to 18 years in boys.
The physeal apex is posteromedial and is associated with a strong, thick periosteum.
Type I physeal fractures occur through the hypertrophic zone adjacent to the zone of provisional calcification. The layer of embryonal cartilage is preserved, leading to normal growth.
Muscular deforming forces: The subscapularis attaches to the lesser tuberosity. The remainder of the rotator cuff (teres minor, supraspinatus, and infraspinatus) attaches to the posterior epiphysis and greater tuberosity. The pectoralis major attaches to the anterior medial metaphysis, and the deltoid connects to the lateral shaft.
Mechanism of Injury
Indirect: Resulting from a fall backward onto an outstretched hand with the elbow extended and the wrist dorsiflexed. Birth injuries may occur as the arm is hyperextended or rotated as the infant is being delivered. Shoulder dystocia is strongly associated with macrosomia from maternal diabetes.
Direct: Resulting from direct trauma to the posterolateral aspect of the shoulder.
Clinical Evaluation
Newborns present with pseudoparalysis with the arm held in extension. A history of birth trauma may be elicited. A fever is variably present. Infection, clavicle fracture, shoulder dislocation, and brachial plexus injury must be ruled out.
Older children present with pain, dysfunction, swelling, and ecchymosis, and the humeral shaft fragment may be palpable anteriorly. The shoulder is tender to palpation, with a painful range of motion that may reveal crepitus.
Typically, the arm is held in internal rotation to prevent anteromedial pull of the distal fragment by the pectoralis major.
A careful neurovascular examination is required, including assessment of the axillary, musculocutaneous, radial, ulnar, and median nerves.
Radiographic Evaluation
Anteroposterior (AP), lateral (in the plane of the scapula; “Y” view), and axillary views should be obtained, with comparison views of the contralateral side if necessary.
Ultrasound: This may be necessary in the newborn because the epiphysis is not yet ossified.
Computed tomography may be useful to aid in the diagnosis and classification of posterior dislocations and complex fractures.
Magnetic resonance imaging is more useful than bone scan to detect occult fractures because the physis normally has increased radionuclide uptake, making a bone scan difficult to interpret.
Classification
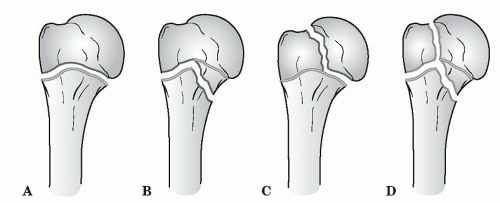
Salter-Harris
- Type I: Transphyseal fracture; usually a birth injury
- Type II: Transphyseal fracture that exits through the metaphysis; usually occurring in adolescents (>12 years old); metaphyseal fragment always posteromedial
- Type III: Transphyseal fracture that exits through the epiphysis uncommon; associated with dislocations
- Type IV: Rare; fracture that traverses the epiphysis and the physis, exiting the metaphysis; associated with open fractures
Neer-Horowitz Classification of Proximal Humeral Plate Fractures
- Grade I: <5 mm displacement
- Grade II: Displacement less than one-third the width of the shaft
- Grade III: Displacement one-third to two-thirds the width of the shaft
- Grade IV: Displacement greater than two-thirds the width of the shaft, including total displacement
Treatment
Treatment depends on the age of the patient as well as the fracture pattern.
Newborns
Most fractures are Salter-Harris type I. The prognosis is excellent.
Ultrasound can be used to guide reduction.
- Closed reduction: This is the treatment of choice and is achieved by applying gentle traction, 90 degrees of flexion, then 90 degrees of abduction and external rotation.
- Stable fracture: The arm is immobilized against the chest for 5 to 10 days.
- Unstable fracture: The arm is held abducted and is externally rotated for 3 to 4 days to allow early callus formation.
Ages 1 to 4 Years
These are typically Salter-Harris type I or, less frequently, type II.
Treatment is by closed reduction.
- The arm is held in a sling for 10 days followed by progressive return to activity.
Extensive remodeling is possible.
Ages 5 to 12 Years
The metaphyseal fracture (type II) is the most common in this age group because this area is undergoing the most rapid remodeling and is therefore structurally vulnerable.
Treatment is by closed reduction. Most are stable following reduction.
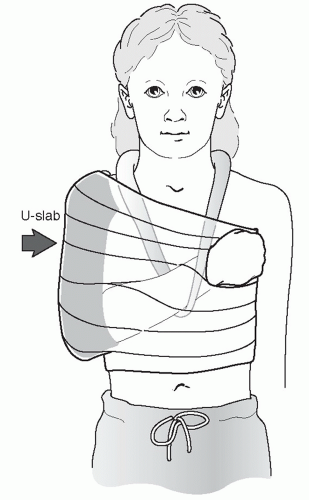
- Stable fracture: A sling and swathe is used (Fig. 43.4).
- Unstable fracture: The arm is placed in a shoulder spica cast with the arm in the salute position for 2 to 3 weeks, after which the patient may be placed in a sling, with progressive return to activity.
Ages 12 Years to Maturity
These are either Salter-Harris type II or, less frequently, type I.
Treatment is typically by closed reduction.
There is less remodeling potential than in younger children.
- Stable fracture: A sling and swathe is used for 2 to 3 weeks followed by progressive range-of-motion exercises.
- Unstable fracture and Salter-Harris type IV: Immobilization is maintained in a shoulder spica cast with the arm in the salute position for 2 to 3 weeks, after which the patient may be placed in a sling, with progressive return to activity.
One should consider surgical stabilization for displaced fractures in adolescents.
Acceptable Deformity
- Ages 1 to 4 years: 70 degrees of angulation with any amount of displacement
- Ages 5 to 12 years: 40 to 45 degrees of angulation and displacement of one-half the width of the shaft
- Ages 12 years to maturity: 15 to 20 degrees of angulation and displacement of <30% the width of the shaft
Open Treatment
Indications for open reduction and internal fixation include:
- Open fractures
- Fractures with associated neurovascular compromise
- Salter-Harris types III and IV fractures with displacement
- Irreducible fractures with soft tissue interposition (biceps tendon)
In children, fixation is most often achieved with percutaneous, smooth Kirschner wires or Steinmann pins.
Prognosis
Neer-Horowitz grades I and II fractures do well because of the remodeling potential of the proximal humeral physis.
Neer-Horowitz grades III and IV fractures may be left with up to 3 mm of shortening or residual angulation. This is well tolerated by the patient and is often clinically insignificant.
As a rule, the younger the patient, the higher the potential for remodeling and the greater the acceptable initial deformity.
Complications
- Proximal humeral varus: Rare, usually affecting patients less than 1 year of age, but it may complicate fractures in patients as old as 5 years of age. It may result in a decrease of the neck-shaft angle to 90 degrees with humeral shortening and mild-to-moderate loss of glenohumeral abduction. Remodeling potential is great in this age group, however, so improvement is likely without intervention. Proximal humeral osteotomy may be performed in cases of extreme functional limitation.
- Limb length inequality: Rarely significant and tends to occur more commonly in surgically treated patients as opposed to those treated nonoperatively.
- Loss of motion: Rare and tends to occur more commonly in surgically treated patients. Older children tend to have more postfracture difficulties with shoulder stiffness than younger children.
- Inferior glenohumeral subluxation: May complicate patients with Salter-Harris type II fractures of the proximal humerus secondary to a loss of deltoid and rotator cuff tone. It may be addressed by a period of immobilization followed by rotator cuff strengthening exercises.
- Osteonecrosis: May occur with associated disruption of the anterolateral ascending branch of the anterior circumflex artery, especially in fractures or dislocations that are not acutely reduced. This is almost never seen in closed fractures.
- Nerve injury: Most commonly axillary nerve injury in fracture-dislocations. Lesions that do not show signs of recovery in 4 months should be explored.
- Growth arrest: May occur when the physis is crushed or significantly displaced or when a physeal bar forms. It may require excision of the physeal bar. Limb lengthening may be required for functional deficits or severe cosmetic deformity.
MCQ Page
Question {{currentIndex + 1}}
{{currentQuestion.question}}
Answer: {{currentQuestion.correctAnswer}}
Explanation: {{currentQuestion.explanation}}