Congenital Vertical Talus Surgery: When is it Necessary?
Learn about the surgical management of congenital vertical talus, including the Dobbs method and extensive soft tissue release, and their respective outcomes and complications.
Summary
Congenital Vertical Talus is a rare congenital condition caused by neuromuscular or chromosomal abnormalities in neonates that typically presents with a rigid flatfoot deformity.
Epidemiology
Incidence: rare, 1:150,000 births
Demographics: M:F ratio of 2:1
Anatomic location: 50% bilateral
Etiology
Pathoanatomy:
- Rigid foot deformity
- Irreducible dorsolateral navicular dislocation
- Vertically oriented talus
- Calcaneal eversion with attenuated spring ligament
- Soft tissue contractures
- Displacement of peroneal longus and posterior tibilais tendon so they function as dorsiflexors rather than plantar flexors
- Contracture of the Achilles tendon
Associated Conditions
50% associated with neuromuscular disease or chromosomal aberrations:
- Myelomeningocele
- Arthrogryposis
- Diastematomyelia
- Congenital dislocation of the hip
- Cerebral palsy
- Spinal muscular atrophy
Presentation
Physical exam:
- Rigid rockerbottom deformity
- Fixed hindfoot equinovalgus
- Rigid midfoot dorsiflexion
- Forefoot abducted and dorsiflexed
- Prominent talar head
- Gait abnormality
- Neurologic deficits

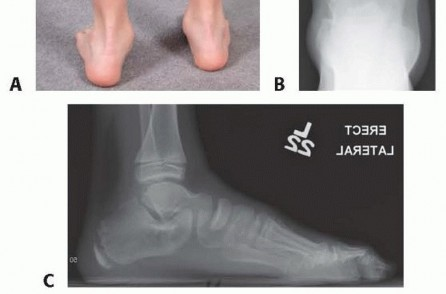
Imaging
Radiographs:
- Recommended views: AP, oblique, and lateral foot
- Findings: [line along long axis of talus passes below the first metatarsal-cuneiform axis
before ossification of navicular at age 3, the first metatarsal is used as a proxy for the navicular on radiographic evaluation]
Differential Diagnosis
Nonoperative: serial manipulation and casting
Treatment
Nonoperative: [insert nonoperative treatment here]
Operative Treatment
| TREATMENT | Description | Indications |
|---|---|---|
| Nonoperative: serial manipulation and casting | Involves manipulating the foot into inversion and plantarflexion, utilizing closed or open pinning of the talonavicular joint with percutaneous Achilles tenotomy. Recommended for individuals seeking to stretch dorsolateral soft-tissue structures preoperatively. | Indicated preoperatively to stretch the dorsolateral soft-tissue structures |
| Operative: surgical release and talonavicular reduction and pinning | Involves pantalar release with concomitant lengthening of peroneals, Achilles, and toe extensors. Talonavicular joint is reduced and pinned while reconstruction of the plantar calcaneonavicular (spring) ligament is performed. Concomitant tibialis anterior transfer to talar neck. Minimally invasive correction. | Indicated in most cases, performed at 6-12 months of age |
| Minimally invasive correction | Utilizes serial casting to stretch contracted dorsal and lateral soft tissue structures gradually. Once reduction is achieved with the cast, closed or open reduction is performed, which is then secured with pin fixation. Percutaneous Achilles tenotomy is required to correct the equinus deformity. | New technique performed in some centers to avoid complications associated with extensive surgical releases |
| Talectomy | Indicated in resistant cases | - |
| Triple arthrodesis | Salvage procedure | - |
Correction Strategy
Correction of all rigid vertical tali is recommended to prevent unfavorable natural history. The Dobbs method of serial manipulation and casting, followed by temporary Kirschner wire stabilization of the talonavicular joint and a tendo Achilles tenotomy, is a treatment strategy that provides excellent correction while avoiding more extensive soft tissue release surgery. Treatment should be initiated during the first 2 months of life if possible, with the goals of providing flexible feet that are plantigrade and functional. Careful consideration should be given to syndromic and/or severely involved neuromuscular patients before initiating treatment.
| Preoperative Planning |
|---|
| The treatment process starting with serial casting should not be initiated with premature infants still in hospital and of low birth weight. These very small patients are difficult to fit into braces which are required to prevent relapse after correction is achieved. The age of the patient is important in preoperative planning, and a tibialis anterior tendon transfer to the neck of talus should be considered for those patients older than 2 years at time of treatment. Neural axis imaging should be performed for those patients in which abnormalities are present, suggestive of spinal pathology. |
Positioning
The patient is positioned supine on a radiolucent table with a nonsterile tourniquet placed on proximal thigh.
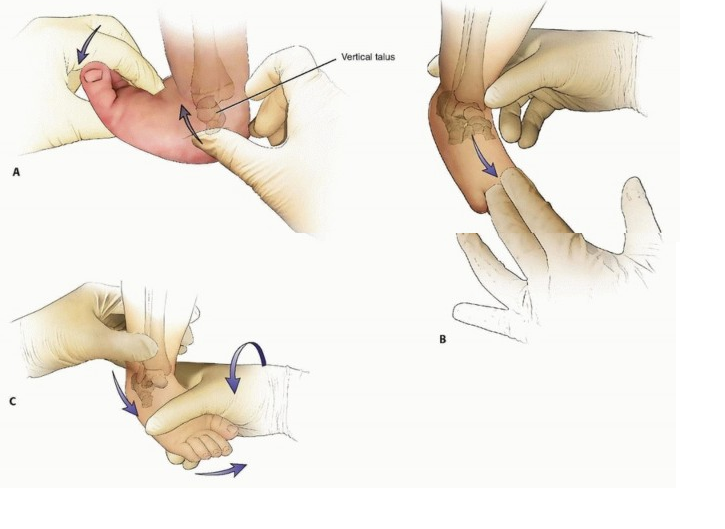
Serial Manipulation - Dobbs Method
The head of the talus is the fulcrum and the point around which the rest of the foot will be manipulated. All components of the deformity are corrected simultaneously with the exception of the hindfoot equinus, which is corrected last. The manipulations are gentle in nature and consist of stretching the foot into plantarflexion and adduction with one hand while counterpressure is applied with the thumb of the opposite hand gently pushing the talus dorsally and laterally. It is essential not to touch the calcaneus during manipulations to prevent the calcaneus from correcting from valgus to varus position. Manipulations are done weekly in the clinic and are gentle in nature. The head of the talus is palpated with the thumb of the examiner, and once identified, direct pressure is placed with the thumb on the head of the talus in a plantar and lateral direction while the examiner, using the other hand, brings the foot into plantarflexion and adduction.
Limited Surgery and Percutaneous Stabilization - Dobbs Method
When reduction is achieved, the patient is scheduled for the operating room for stabilization of the talonavicular joint with a Kirschner wire followed by a percutaneous tendo Achilles tenotomy. In the operating room, a small 1-cm incision is made dorsomedially over the talonavicular joint. This allows the surgeon, without opening the joint capsule in most cases, to ensure the talonavicular joint is reduced and aids in Kirschner wire placement. Once the talonavicular joint is reduced, a smooth 0.062-mm Kirschner wire is placed in a retrograde manner across the joint under direct visualization and confirmed radiographically. Once the talonavicular joint is stabilized, a tenotomy is done of the tendo Achilles to correct residual equinus. A long-leg cast is applied with the ankle and forefoot in a neutral position.
Extensive Soft Tissue Release
A dorsal approach is used to perform a talonavicular capsulotomy and lengthening of the tibialis anterior tendon, extensor digitorum longus, and peroneal tendons, as well as capsulotomies of the subtalar joint both medially and laterally. A posterior incision is performed next to lengthen the Achilles tendon and release the posterior subtalar and ankle joints. The talonavicular joint is then reduced, held with a Kirschner wire, and the calcaneocuboid joint is released if subluxation of this joint is still present. This is also held reduced with a Kirschner wire.
Postoperative Care
The cast is changed 2 weeks postoperatively to manipulate the ankle to 10 degrees of dorsiflexion, and the pin is removed in the operating room at 6 weeks from the index procedure. The patient is placed in a dynamic shoe and bar brace system, which they are to wear 23 hours a day for 2 months and then at nighttime for 2 years to prevent relapse. The shoes on the brace are set pointing ahead to stretch the peroneal tendons. The dynamic bar allows active motion at the knees and ankles and also encourages active plantarflexion stretching of the dorsolateral soft tissues. Follow-up is at 1 month after initiating brace wear and then every 3 months for the first 2 years. After that, follow-up is yearly for several years and then every 2 years until the age of 8 years.
Outcomes
The Dobbs method has been shown in multiple studies from around the world to allow excellent clinical and radiographic correction in isolated and nonisolated (syndromic and neuromuscular) cases. A recent study comparing the Dobbs method with traditional extensive soft tissue release surgery demonstrated that while both methods achieve good radiographic correction, the Dobbs method provides superior clinical and functional results as measured by better subtalar and ankle range of motion and less pain with growth.
Complications
Complications may include skin complications from casting, Kirschner wire back out from soft cartilaginous structures, difficulties with postoperative bracing, avascular necrosis of talus, wound dehiscence, undercorrection, overcorrection, ankle and subtalar joint stiffness, vascular and neurologic injuries.