"Finger Replantation: Restoring Form and Function after Traumatic Amputation
Learn about the epidemiology, pathophysiology, indications, treatment, and postoperative care for finger replantation after traumatic amputations. Restore form and function with this complex surgical technique.
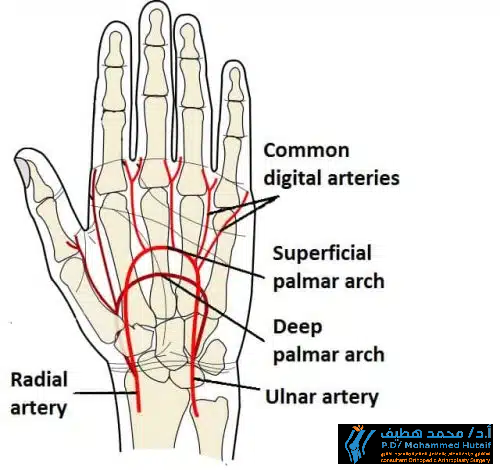
Introduction
Finger replantation is the reattachment and reconstruction of an amputated portion of a digit. It aims to restore the amputated part to its anatomical site, preserving form and function. Most upper extremity amputations occur secondary to trauma.
Upon complete amputation, the amputated part is without blood supply and starts to become ischaemic. Depending on preservation of this part, ischaemic tolerance times can vary from 12 hours if warm or to 24 hours if cold.
Digital amputations generally have longer ischaemic tolerance times than proximal limb amputations because they have less muscle (which undergoes irreversible damage after 6 hours).
Epidemiology
- Incidence - 90% of upper extremity amputation occurred after trauma
- Demographics - 4:1 male-to-female ratio
- Anatomic location - most amputations occur at the level of the digits
Pathophysiology
Mechanism of traumatic amputation:
- Sharp dissection
- Blunt dissection
- Avulsion
- Crush
Presentation
History:
- Timing of injury
- Type and location of amputation
- Number of digits involved
- Preservation of amputated tissue
- Associated injury
- Past medical history
Examination:
- Stump examined for:
- Zone of injury
- Tissue viability
- Supporting tissue structures
- Contamination
- Amputated portion inspected for:
- Segmental injury
- Bone and soft tissue envelope
- Contamination
Indications
Indications for replantation after trauma:
- Primary indications
- Thumb at any level
- Multiple digits
- Through the palm
- Wrist level or proximal to wrist
- Almost all parts in children
- Relative indications
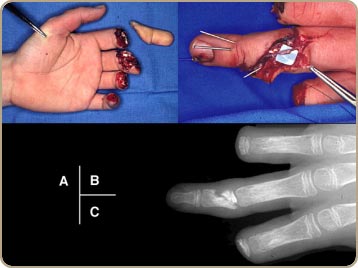
- Individual digits distal to the insertion of flexor digitorum superficialis [FDS] (Zone I)
- Ring avulsion
- Through or above elbow
- Contraindications to replantation
- Primary contraindications
- Severe vascular disorder
- Mangled limb or crush injury
- Segmental amputation
- Prolonged ischemia time with large muscle content (>6 hours)
- Relative contraindications
- Single digit proximal to FDS insertion (Zone II)
- Ring finger injuries in zone II have better cosmesis and grip strength with 4th ray resection and 5th ray transposition
- Medically unstable patient with finger replantation surgery
- Disabling psychiatric illness
- Tissue contamination
- Prolonged ischemia time with no muscle content (>12 hours)
Treatment
Transport of amputated tissue:
- Indications
- Any salvageable tissue should be transported with the patient to hospital
- Modality
- Keep amputated tissue wrapped in moist gauze in lactate ringers solution
- Place in sealed plastic bag and place in ice water (avoid direct ice or dry ice)
- Wrap, cover and compress stump with moistened gauze
Operative:
- Time to replantation
- Proximal to carpus
- Warm ischemia time < 6 hours
- Cold ischemia time < 12 hours
- Distal to carpus (digit)
- Warm ischemia time < 12 hours
- Cold ischemia time < 24 hours
- General operative sequence of replantation
- Vascular shunt first (for proximal replantation with large muscle mass to minimize warm ischemia time)
- Bone fixation +/- shortening (after irrigation and debridement of soft-tissue and bone)
- Extensor tendon repair
- Artery repair (repair second after bone if ischemic time is >3-4 hours)
- Venous anastomoses
- Flexor tendon repair
- Nerve repair
- Skin +/- fasciotomy
- Finger order
- Thumb, long, ring, small, index
- For multiple amputations structure-by-structure sequence is most efficient
- Digit-by-digit sequence takes the most time
Postoperative Care
- Environment
- Keep patient in warm room (80°F)
- Avoid caffeine, chocolate, and nicotine
- Replant monitoring
- Skin temperature most reliable
- Concerning changes include a > 2° drop in skin temp in less than one hour or a temperature below 30° Celsius
- Pulse oximetry
- < 94% indicates potential vascular compromise
- Anticoagulation
- Adequate hydration
- Medications (aspirin, dipyridamole, low-molecular weight dextran, heparin)
- Arterial Insufficiency
- Treat with:
- Release constricting bandages
- Place extremity in dependent position
- Consider heparinization
- Consider stellate ganglion blockade
- Early surgical exploration if previous measures unsuccessful
- Thrombosis secondary to vasospasm is most common cause of early replant failure
- Venous congestion
- Treatment
- Elevate extremity
- Leech application
- Releases Hirudin (powerful anticoagulant)
- Aeromonas hydrophila infection can occur
- Prophylaxis with Ciprofloxacin or Bactrim
- Heparin soaked pledgets if leeches not available
Complications
- Replantation failure
- Most frequently cause within 12 hours is arterial thrombosis from persistent vasospasm
- Decreased palmar width with ray resection
- Stiffness
- Replanted digits have 50% of total motion
- Tenolysis is most common secondary surgery
- Myonecrosis
- Greater concern in major limb replantation than in digit replantation
- Myoglobinuria
- Caused by muscle necrosis in larger replants (forearm and arm)
- Can lead to renal failure and be fatal
- Reperfusion injury
- Mechanism thought to be related to ischemia-induced hypoxanthine conversion to xanthine
- Allopurinol is the best adjunctive therapy agent to decrease xanthine production
- Infection
- Cold intolerance
"Maximizing Success for Finger Replantation: Understanding Ischemic Tolerance Times and Operative Sequence" Discover the optimal time frame for finger replantation, dependent on location and ischemic tolerance time. Learn about the general operative sequence and the various surgical techniques used to maximize success for this complex procedure.