Proper Exposure and Precise Reduction: Treating Distal Tibia Fractures
Learn about the standard anterior approach and medial approach for SER fractures and how to achieve accurate reduction by identifying and protecting the growth plate and periosteum.
Exposure and Reduction
The previously described standard anterior approach for SER fractures is utilized.
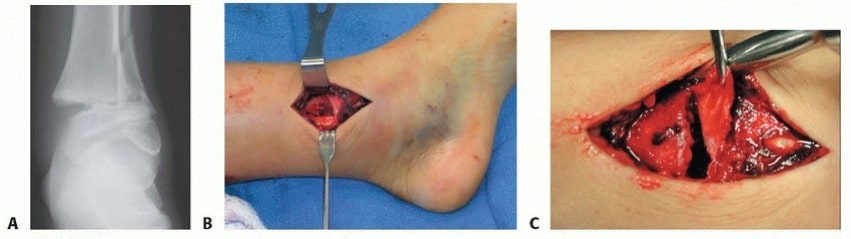
For a Salter-Harris type II abduction injury with medial gapping, a medial approach is employed (TECH FIG 1).
The exact location of the fracture determines whether the approach should be slightly more medial or lateral.
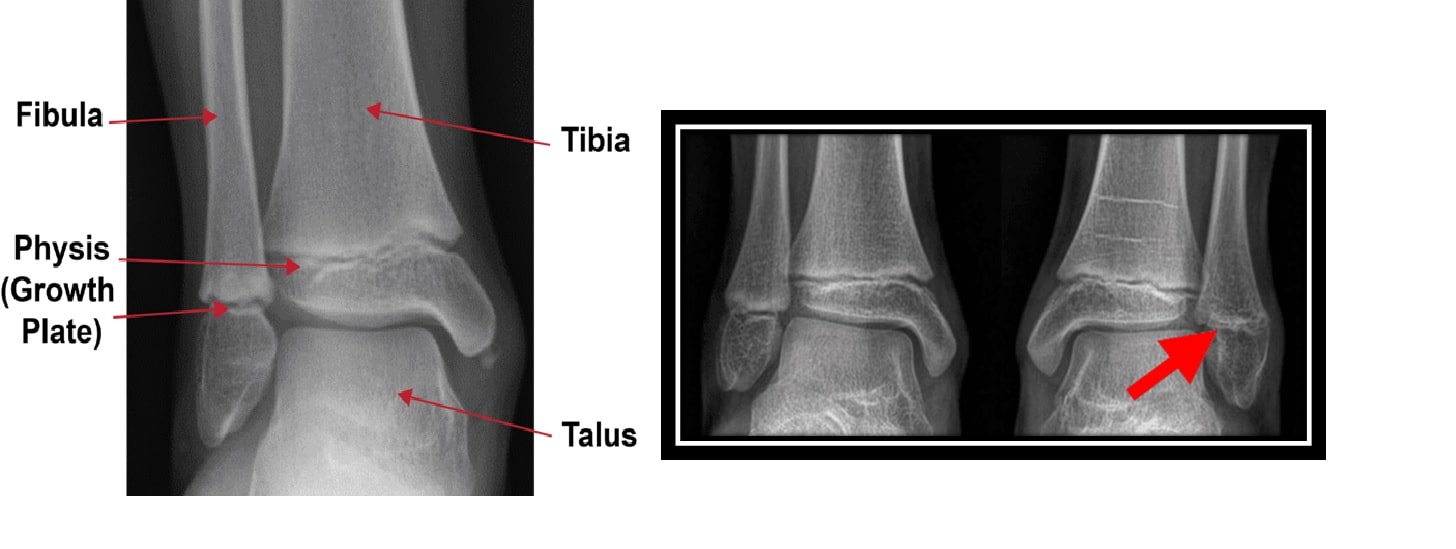
Identification and definition of the fracture and growth plate is necessary.
The perichondral ring and growth plate must be identified and protected.
The physis displays a distinctive white cartilaginous appearance.
Placement of two Hohmann-type retractors around the distal tibia allows for proper exposure.
Once exposure is achieved, the interposed periosteum can be carefully eliminated using a Freer elevator.
Preservation of periosteum is important as it supports blood flow for fracture healing and is closely associated with the perichondral ring.
The periosteum may be cautiously incised to facilitate its removal from the fracture site and achieve accurate reduction.
Once the periosteum is removed without causing trauma, the reduction becomes relatively easy and the fracture is typically stable.
Stabilization
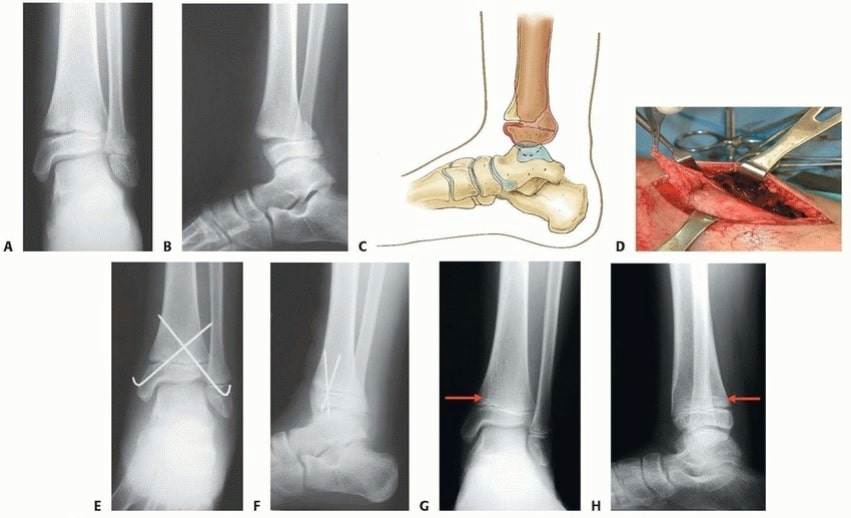
Many Salter-Harris type II fractures can be successfully stabilized using two 0.062-inch smooth Kirschner wires.
The wires are inserted from distal to proximal, starting from the anteromedial malleolus and the anterolateral corner of the tibial epiphysis (TECH FIG 2).
The percutaneous pins must be inserted distally enough through the skin to reach the appropriate starting point in the bone.
During insertion, the Kirschner wires can be observed directly through the open incision as they enter the bone.
In some cases, large metaphyseal fragments may require more appropriate stabilization using one or two lagged cancellous bone screws.
These screws should be placed proximal to the physis and perpendicular to the fracture site.
Alternatively, cannulated screws can be used based on the surgeon's preference.
Key Points:
- Ankle fractures in children can be categorized into different types according to the Salter-Harris classification.
- The standard anterior approach is typically used for SER fractures.
- For Salter-Harris type II abduction injuries with medial gapping, a medial approach is employed.
- The perichondral ring and growth plate must be identified and protected during surgery.
- Two Hohmann-type retractors are used to properly expose the distal tibia.
- The periosteum, which supports blood flow for fracture healing, should be preserved but can be carefully removed for accurate reduction.
- Two 0.062-inch smooth Kirschner wires are often used for stabilization of Salter-Harris type II fractures.
- Percutaneous pins must be inserted distally enough to reach the appropriate starting point in the bone.
- Large metaphyseal fragments may require stabilization using lagged cancellous bone screws placed proximal to the physis and perpendicular to the fracture site.
- Alternatively, cannulated screws can be used depending on the surgeon's preference.