
AO sacral fracture classification
1. Introduction
The classification system described here exists in order to provide surgeons from different institutions with a common language to discuss various injuries. It provides consistency in injury diagnosis and treatment.
The AOSpine sacral fracture classification system aims to achieve international acceptance.
The classification system describes injuries based on three criteria:
morphology of the injury
neurologic status
case-specific modifiers
Each criterion is described below. Injuries are described by the morphologic type of the primary injury. The secondary injuries and modifiers are placed in parentheses (facet injury, neurologic status, and case specific modifiers).
2. Morphology of the injury
Three basic categories (Types) were used to describe primary injury morphology.
Type A injuries are lower sacro-coccygeal fractures which have no impact on the posterior pelvic or spino-pelvic stability.
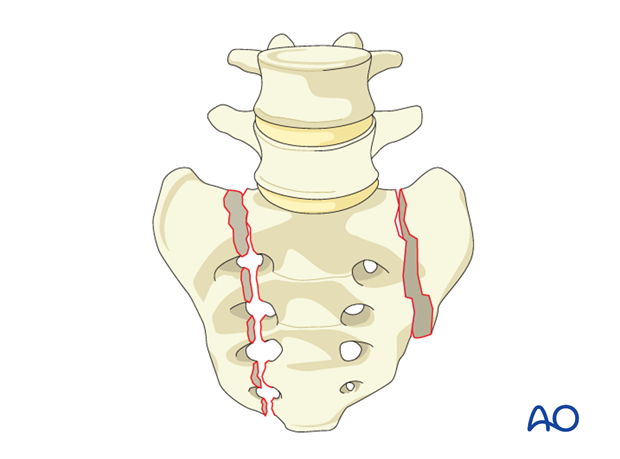
Type B injuries are unilateral longitudinal (vertical) sacral fractures which primarily result in posterior pelvic instability. There is no impact on spino-pelvic stability. These injuries have also been classified as Denis Zone I through III.
Type C injuries include unilateral B injuries with L5-S1 facet involvement, bilateral longitudinal (vertical) sacral fractures and U fracture variations resulting in spino-pelvic instability. Sacral U-fracture variations have also been classified according to Roy-Camille.
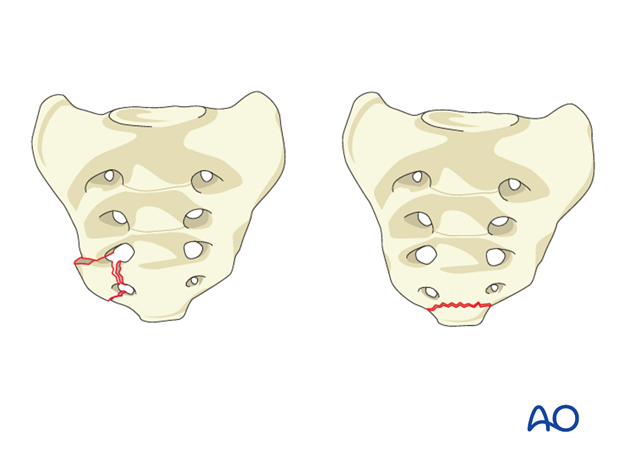
3. A1
These are either coccygeal/sacral compression fractures or ligamentous avulsion fractures.
4. A2
This is a nondisplaced transverse fracture below the SI-Joint with a low likelihood of cauda equina injury.
5. A3
This is a displaced transverse fracture below the SI-Joint which has a higher likelihood of neurological injury than A1 and A2.
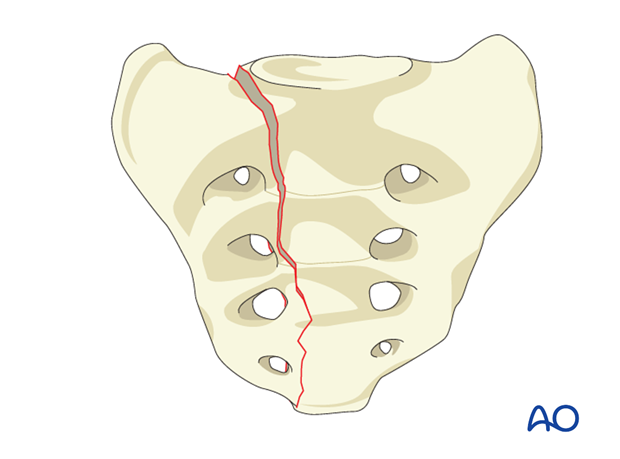
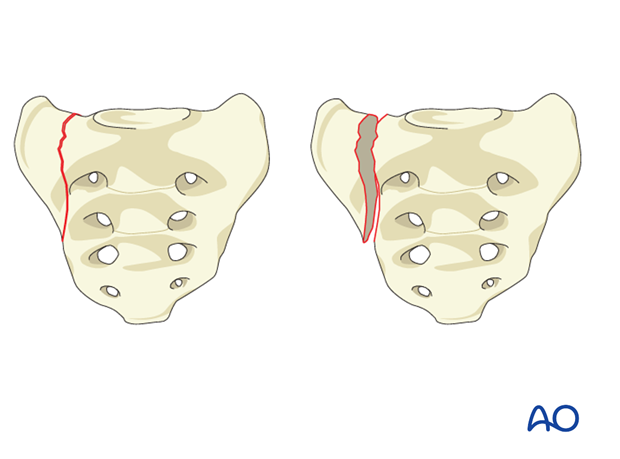
6. B1
This is a longitudinal central facture of the sacrum involving the spinal canal, but with a very low likelihood of neurological injury. B1 fractures correspond to Denis Zone III injuries.
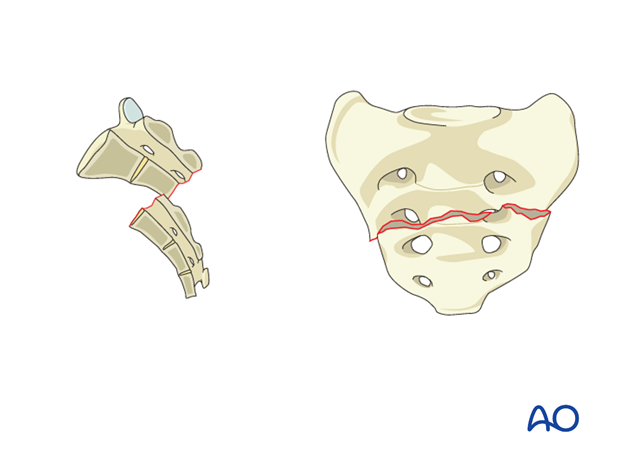
 7. B2
7. B2
This is a transalar fracture which does not involve the foramina or the spinal canal. There is approximally 5% chance of neuro injury (primarily L5 where the L5 root can get trapped between the displaced sacral ala and L5 transverse process). B2 fractures correspond to Denis Zone I injuries.
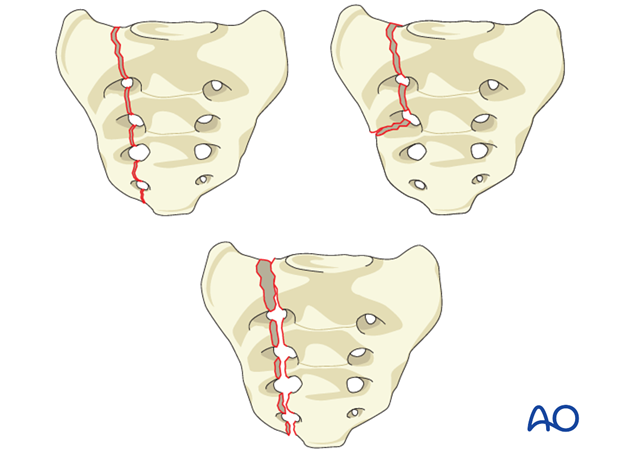
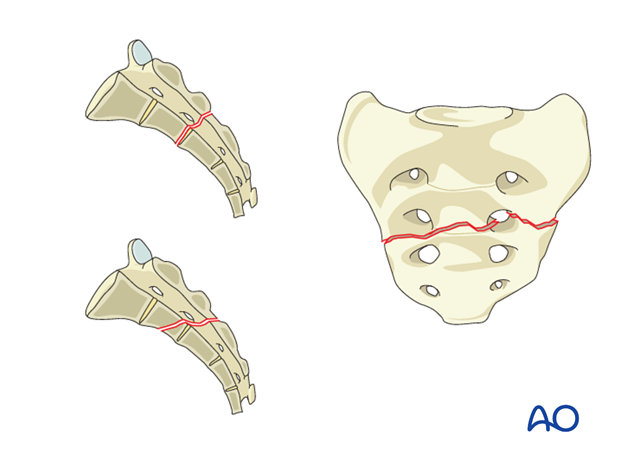
8. B3
This is a transforaminal fracture which does not involve the spinal canal. There is approximally 25% chance of neuro injury. B2 fractures correspond to Denis Zone II injuries.
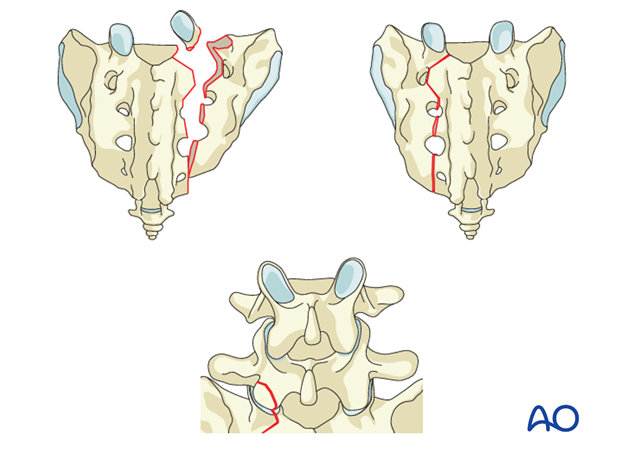
9. C0
This is a nondisplaced sacral U-type fracture, typically resulting from low-energy injuries. These injuries are most commonly seen as insufficiency fractures in patients with metabolic bone disease.
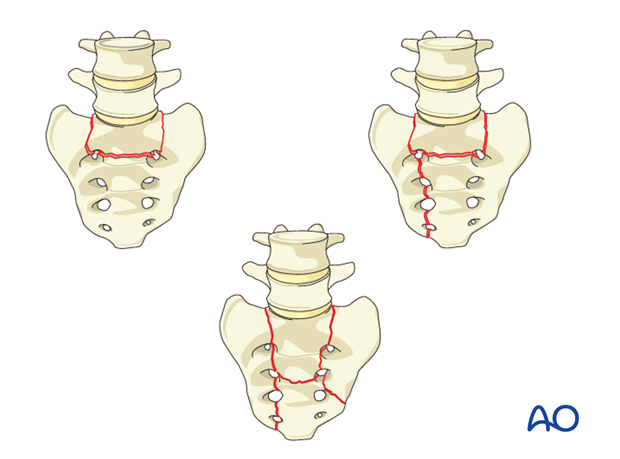
10. C1
This is any unilateral B-type fracture involving a fracture of the ipsilateral L5-S1 joint. This fracture type may impact spino-pelvic instability and is therefore classified as a C fracture.
11. C2
This is a bilateral B-type fracture without a transverse component. These fractures are more unstable and have a higher risk of neurological injury than C1.
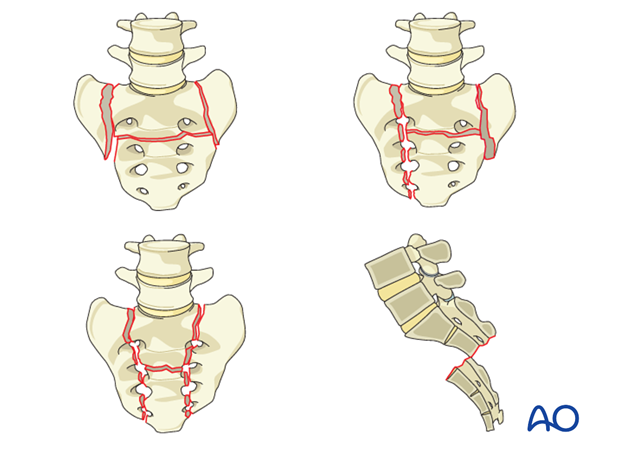
12. C3
This is a displaced U-type fracture. It has a similar instability profile as C2, but due to the transverse fracture displacement it has a higher likelihood of neurological injury.
13. Neurology
Neurological injuries are classified as follows:
Nx: Cannot be examined
N0: No neurological deficits
N1: Transient neurological injury
N2: Nerve root injury
N3: Cauda Equina Syndrome/Incomplete SCI
N4: Complete SCI*
* The AO Spine Injury Classification Systems follow a universal neurological system for the whole spine. For the sacrum, N4 is theoretically and anatomically impossible.
14. Modifiers
These modifiers are added to distinguish features that may impact treatment of a given fracture type.
M1: Severe soft Tissue Injury
M2: Metabolic Bone Disease
M3: Anterior pelvic ring injury
M4: Sacroiliac joint injury