
Fractures of the Medial Epicondyle
Open Reduction and Internal Fixation of Fractures of the Medial Epicondyle
DEFINITION
■Trauma to the medial aspect of the elbow may cause a me- dial epicondyle fracture, which is an injury to the apophysis of the medial epicondyle.
ANATOMY
■Medial epicondylar fractures involve the medial epicondylar apophysis on the posteromedial aspect of the elbow.
■The flexor–pronator muscle mass arises from this apoph- ysis, including the palmaris longus, the flexor carpi ulnaris and radialis, the flexor digitorum superficialis, and one part of the pronator teres and the ulnar collateral ligament (FIG 1).3
PATHOGENESIS
■A direct blow to the medial aspect of the elbow may cause a fracture to the medial epicondyle, but this is rare.
■More commonly, a fall on an outstretched arm causes an avulsion of the medical epicondyle via tension generated by stretch of the muscles attaching to it. Elbow dislocation is fre- quently associated with a medial epicondyle fracture and may occur with spontaneous reduction at the time of the injury (FIG 2).
■Considerable force applied to the arm may cause elbow dis-
location and associated disruption of the ulnar collateral liga- ment. This ligament, the principal stabilizing ligament of the elbow, can avulse the medial epicondyle, and the apophyseal fragment may sometimes become lodged in the elbow joint.3
■Overuse may cause a chronic stress-type injury or an apophysitis, an example of which would be Little League elbow.
NATURAL HISTORY
■The outcome of medial epicondyle fractures is related to the amount of fracture displacement and also the demands placed on the elbow by the patient.
■Minimally displaced fractures treated nonoperatively gener- ally do well, especially if the patient is not an athlete or if the fracture involves the patient’s nondominant arm.
■Untreated displaced fractures may lead to chronic medial elbow instability and even recurrent elbow dislocations.
■Throwing athletes may have significant impairment in their sports activities.5
PATIENT HISTORY AND PHYSICAL FINDINGS
■For any elbow injury, the mechanism of injury should be sought, with particular attention to the details of a fall. In chil- dren this may be difficult to elicit, but often a witness may be available. Medial epicondyle fractures frequently arise from a fall.
■The two most important issues in the physical examination are to document neurovascular status and to assess for elbow stability. Determination of stability includes determination of whether the elbow is dislocated, which can be assessed clini- cally and confirmed radiographically.
■Assessment of medial elbow stability is often important in determining treatment.
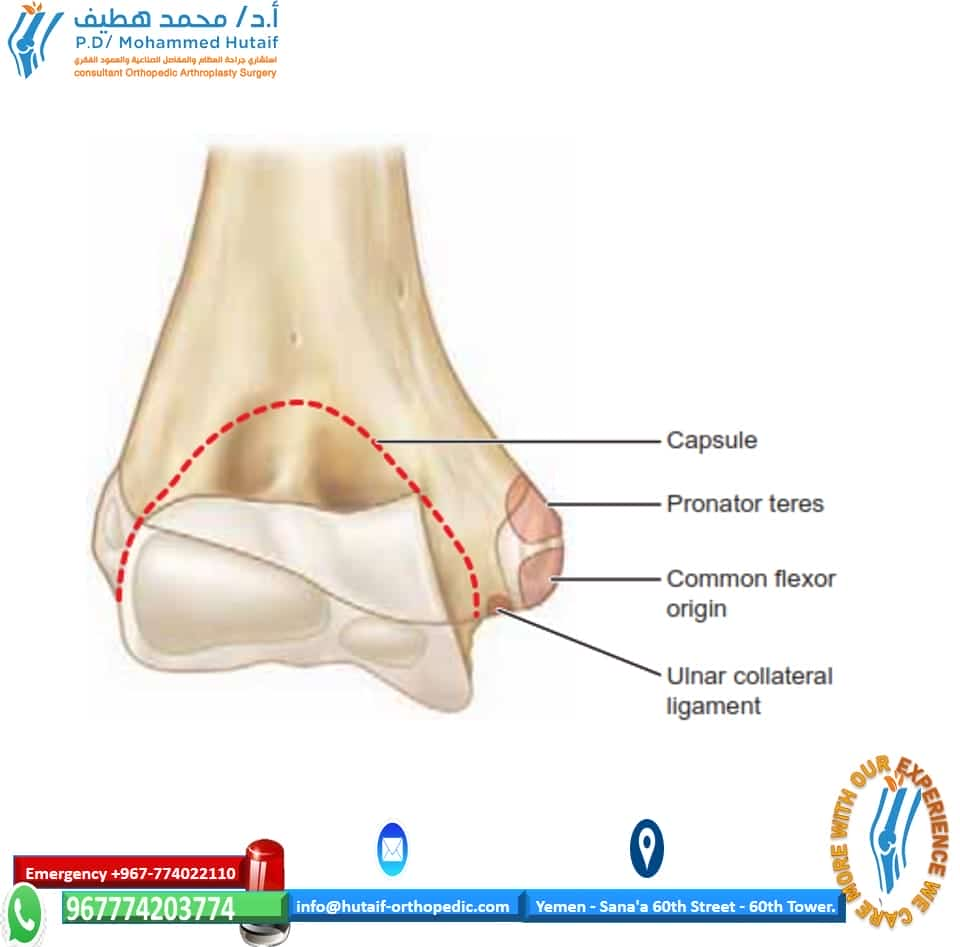
FIG 1 • Anatomic landmarks and site of muscle and ligament attachments on medial epicondyle.
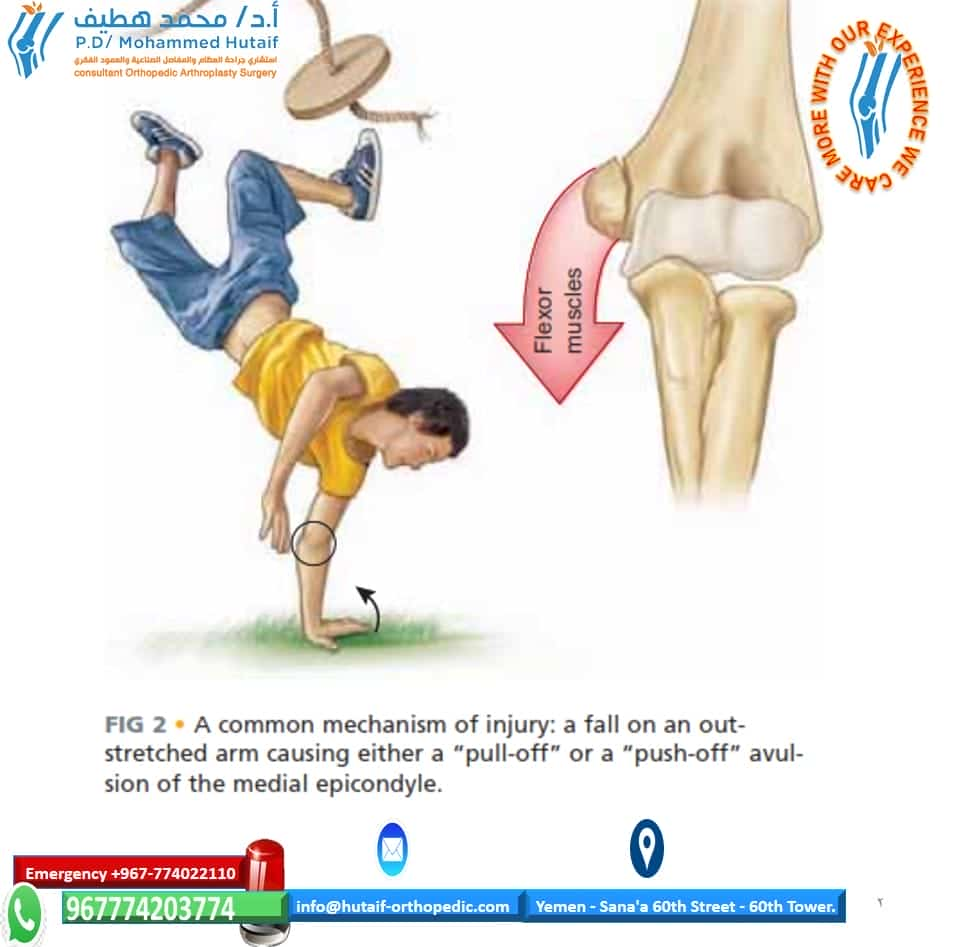
FIG 2 • A common mechanism of injury: a fall on an out- stretched arm causing either a “pull-off” or a “push-off” avul- sion of the medial epicondyle.
■A positive valgus stress test confirms medial elbow instabil- ity. Persistence of medial elbow stability may cause significant elbow disability in athletes or those doing heavy labor. Radiographs may confirm increased displacement of the me- dial epicondylar fragment.
IMAGING AND OTHER DIAGNOSTIC STUDIES
■Standard anteroposterior (AP) and lateral radiographs of the elbow are required, but oblique views are often helpful to visualize the medial epicondyle, which is on the posteromedial aspect of the distal humerus.
■Widening of the apophysis may be the only sign of injury, so comparison views of the unaffected elbow are often helpful to assess for amount of displacement.
■If there is radiographic absence of the medial epicondyle and suspected joint incarceration, an arthrogram, CT scan, or MRI may be needed rarely.
DIFFERENTIAL DIAGNOSIS
■Medial condylar fractures
■Supracondylar fractures
■Elbow dislocation
NONOPERATIVE MANAGEMENT
■Smith in 1950 became a strong advocate of nonoperative management of this injury, pointing out that the fracture in- volved an apophysis rather than a physis, and thus future growth was not compromised. He also documented that im- perfect reduction or even nonunion was not automatically as- sociated with a poor outcome in terms of elbow function and strength.3
■A recent study from Sweden where all patients were treated nonoperatively showed 96% good to excellent results. Over
60% of the patients had a fibrous union or nonunion.3
■Two studies have compared nonoperative and operative treatment. Bede and associates1 found that nonoperative treat- ment had better outcomes than operative treatment.
■Farsetti and coworkers4 demonstrated similar results in
displaced fractures of nonoperative treatment and open reduction and internal fixation (ORIF) with Kirschner wires.
■Indications for nonoperative management of medial epi- condyle fractures include patients who do not place high phys- ical demands on their elbows, and most nondominant elbows.
■Nonoperative treatment encompasses splinting for 5 to 7 days or until acute soft tissue swelling resolves and then early active range of motion starting as soon as possible after the injury.
■Physical therapy may be required if range of motion is slow to return, but passive stretch may cause more injury and should be avoided.
SURGICAL MANAGEMENT
■Absolute indications
■Incarceration of the medical epicondylar fragment in the joint
■ Associated elbow dislocation with ulnar nerve dysfunction
FIG 3 • Injury film. The medial epicondylar fragment is displaced and located in the joint.
■Relative indications
■Elbow dislocation in a high-demand patient
■A displaced fracture with medial elbow instability in a high-demand patient
Preoperative Planning
■Careful review of radiographs is done to assess the elbow joint for reduction and to assess the amount of displacement of the medical epicondylar fracture (FIG 3).
■A complete assessment of neurovascular status of the upper
extremity is performed, with particular attention to the ulnar nerve examination.
■A valgus stress test is performed to assess for medial elbow instability, typically under sedation or anesthesia.
Positioning
■The patient is placed supine on the operating table with the arm abducted 90 degrees at the shoulder and placed on a radi- olucent hand table. The arm is externally rotated such that the medial aspect of the elbow is accessible (FIG 4).
■Alternatively, a C-arm image intensifier base may serve as
the operating table for a smaller child or based on the surgeon’s preference.
■The surgeon should be positioned in the patient’s axilla for surgery.
FIG 4 • Arm positioning and approach to the medial epicondyle, with the ulnar nerve course marked out.
OPEN REDUCTION AND INTERNAL FIXATION WITH CANNULATED SCREW
■A skin incision about 4 cm long is made centered over the medial epicondyle after inflation of a tourniquet on the upper arm (TECH FIG 1A). Often with displaced injuries, the fractured fragment is just subcutaneous and little dissection is required.
■The ulnar nerve should be identified and carefully pro-
tected. Most experts do not recommend routine mobi- lization or transposition of the nerve.
■The fracture is identified and any organized hematoma
is removed (TECH FIG 1B).
■The fracture is reduced with a towel clip. Elbow flexion and forearm pronation aid in reducing the fracture.
■Some surgeons suggest curettage of the apophyseal car-
tilage to expedite healing of the fracture, which may persist as a healed apophysis if this is not done. This tip may be especially advantageous in the throwing athlete who is eager to return to sports as soon as possible.
■The fracture is stabilized with one or two guide pins
from the 4.0 cannulated screw set.
■Radiographs are checked to assess reduction and pin placement.
■The pin selected for overdrilling should not be in the ole-
cranon fossa. The second pin provides rotational stability of the fragment during drilling and screw placement.
■An appropriate-length screw is selected and inserted
over the guide pin, stabilizing the fracture.
■ A washer may be used to provide a wide surface area of fixation and prevent screw head migration.
■AP and lateral intraoperative radiographs should con-
firm reduction and screw placement position (TECH FIG
1C–G).
■Elbow stability should be checked and full range of mo- tion confirmed before closure.
■Standard skin closure is carried out, and the arm is
splinted or casted at 90 degrees of elbow flexion.

TECH FIG 1 • A. Incision with ulnar nerve identified. B. The fracture fragment is mobilized. C. Fluoroscopic image showing two pins spanning the fracture fragment for rotational stability. D,E. Cannulated screw fixation shown fluoroscopically. F,G. Radiographs showing healed fracture. Heterotopic bone formation anteriorly can be seen on the lateral radiograph.
SUTURE FIXATION
■Should the fracture cause comminution of the medial epicondyle, repair with sutures may be warranted in a high-demand patient or one with medial instability.
■This would involve sutures placed directly in the tendi- nous tissue and secured to the periosteum adjacent to the bed from which the epicondyle was avulsed.
EXTRACTION OF MEDIAL EPICONDYLE FROM ELBOW JOINT: ROBERTS TECHNIQUE
■A valgus stress is applied to the elbow with the forearm supinated.
■The wrist and fingers are dorsiflexed.
■As the position is reached, the fragment should be dis- lodged from the joint.
■This technique is most effective in the first 24 hours after
the injury, before much muscle spasm occurs.3
PEARLS AND PITFALLS
Medial epicondyle fracture fragment should be fixed ■ The surgeon must beware of a medial epicondyle that is with a cannulated screw if possible rather than pins to have absent on radiography: it may be trapped in the joint. rigid fixation permitting early motion.
Elbow motion is encouraged as soon as possible after surgery ■ The surgeon must document radiographically that the
to minimize postoperative stiffness. internal fixation is not in the olecranon fossa, where it may block elbow extension.
POSTOPERATIVE CARE
■Postoperative management after open reduction of medial epicondyle fractures depends on the type and stability of the fixation of the epicondylar fragment.
■For ORIF with screws, initial splinting for 3 to 5 days in about 50 to 60 degrees of flexion is recommended, followed by early active range of motion.
■Some authors recommend a removable brace preventing val- gus stress but permitting full flexion and extension for 4 weeks.2
■In one recent series on young athletes with this injury re- paired with screw fixation, active range of motion out of the brace continued from weeks 5 to 8 postoperatively. At 8 weeks noncontact sports were allowed, and return to full activity was possible at 12 weeks after surgery.2
OUTCOMES
■Eight adolescent athletes undergoing ORIF with screw fixa- tion for this fracture had excellent results with no residual val- gus instability and full return to all sports. One patient had a loss of 5 degrees of hyperextension, but all other patients had recovery of full range of motion.2
■In another series, 21 of 23 patients treated operatively had recovery of full movement, whereas only 14 of 20 patients treated nonoperatively had full range of motion.6
■A recent series of operative treatment and early motion in
25 patients with displaced fractures showed good to excellent results in all patients.5
COMPLICATIONS
■Failure to diagnose joint entrapment of the medial epi- condyle fracture
■Ulnar nerve dysfunction
■Loss of range of motion
■Nonunion
■Myositis ossificans
REFERENCES
1. Bede WB, Lefebure AR, Rosman MA. Fractures of the medial humeral epicondyle in children. Can J Surg 1975;118:137–142.
2. Case SL, Hennrikus WL. Surgical treatment of displaced medial epi- condyle fractures in adolescent athletes. Am J Sports Med 1997;25:
682–686.
3. Chambers HG, Wilkins KE. Medial apophyseal fractures. In
Rockwood CA, Wilkins KE, Beaty JH, eds. Fractures in Children, ed
6. Philadelphia: Lippincott-Raven, 1996:800–819.
4. Farsetti P, Potenza V, Caterini R, et al. Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;84A:1299–1305.
5. Lee HH, Shen HC, Chang JH, et al. Operative treatment of displaced medial epicondyle fractures in children and adolescents. J Shoulder Elbow Surg 2005;14:178–185.
6. Wilson NI, Ingram R, Rymaszewski L, et al. Treatment of fractures of the medial epicondyle of the humerus. Injury 1988;19:342–344.