
Surgical Approaches to the Shoulder and Elbow
Surgical Approaches to the Shoulder and Elbow
SHOULDER APPROACHES
ANTERIOR APPROACH TO THE SHOULDER
Indications
■ Surgical stabilization for recurrent dislocations
■ Subscapularis and biceps tendon repair
■ Shoulder arthroplasty
■ Fracture fixation
Incisions
■ Anterior shoulder can be approached through two different incisions.
■ Anterior incision:
■ 10- to 15-cm incision along the deltopectoral interval
(FIG 1A)
■ Incision begins just above the coracoid process and pro- gresses toward the deltoid tuberosity.
■ Axillary incision
■ Vertical incision 8 to 10 cm long (FIG 1B)
■ Incision begins inferior to the tip of the coracoid and pro- gresses toward the anterior axillary fold.
Internervous Plane
■ Deltoid muscle is supplied by the axillary nerve.
■ Pectoralis major muscle is supplied by medial and lateral pectoral nerves.
Surgical Dissection
■ Skin flaps are developed around the deltopectoral interval.
■ The deltopectoral interval, with its cephalic vein, is identified.
■ The deltopectoral interval is developed by retracting the pec- toralis major medially and the deltoid laterally.
■ Vein may be retracted either medially or laterally.
■ We prefer to take it laterally, as fewer tributaries are disrupted.
■ The lateral border of the conjoint tendon is identified and the short head of the biceps (supplied by the musculocuta- neous nerve) and coracobrachialis (supplied by the musculocu- taneous nerve) are displaced medially to allow access to the anterior aspect of the shoulder joint.
■ Simple medial retraction of the conjoined tendon may be enough for a procedure such as subscapularis repair or cap- sular repair.
■ If more exposure is necessary, the conjoint tendon can be detached with the tip of the coracoid process.
■ The axillary artery is surrounded by cords of brachial plexus, which lie behind the pectoralis minor muscle.
■ To minimize risk for nerve injury, the arm should be kept adducted while work is being done around the coracoid process.
■ Remember, the musculocutaneous nerve enters the cora- cobrachialis on its medial side.
■ Overly aggressive retraction can cause a neurapraxia of the musculocutaneous nerve.
■ Behind the conjoined tendon of the coracobrachialis and the short head of biceps lies the subscapularis muscle.
■ Externally rotating the arm brings the subscapularis further into the operative field.
■ This maneuver increases the distance between the sub- scapularis and axillary nerve as it disappears below the lower border of the muscle.
■ Identifiable landmarks on the inferior border of the sub- scapularis are three small vessels (from the anterior humeral circumflex artery) that run transversely and often require liga- tion or cauterization.
■ These vessels run as a triad (often called the “three sisters”):
a small artery with its two surrounding venae comitantes.
■ The superior border of the subscapularis muscle blends in with the fibers of the supraspinatus muscle in the rotator inter- val (FIG 1C).
■ The tendon of the subscapularis is tagged with stay sutures.
■ There are various ways of taking down the subscapularis as per surgeon preference.
■ Some divide the subscapularis 1 to 2 cm from its inser- tion onto the lesser tuberosity.
■ Some detach this insertion with a small flake of bone using an osteotome.
■ Inferior border of the subscapularis is the easiest location to allow separation between the subscapularis and capsule.
■ The capsule is incised longitudinally to enter the joint wher- ever the selected repair must be performed.
ANTEROSUPERIOR APPROACH TO THE SHOULDER
Indications
■ Rotator cuff repair
■ Subacromial decompression of the shoulder
■ Acromioclavicular reconstructions
■ Greater tuberosity fractures
■ Removal of calcific deposits from the subacromial bursa
■ Reverse shoulder replacement
Incision
■ An incision is made paralleling the lateral acromion that be- gins at the anterolateral corner of the acromion and ends just lateral to the tip of the coracoid (FIG 2A).
Internervous Plane
■ The deltoid muscle is detached proximal to its nerve supply; therefore, there is no internervous plane with this approach.
Surgical Dissection
■ The incision is deepened to the deep deltoid fascia.
■ Subcutaneous flaps are raised.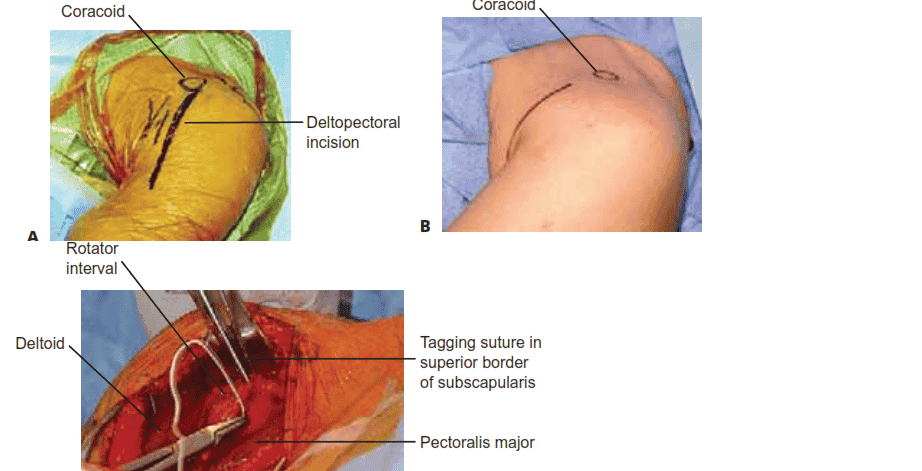
C
FIG 1 • A. Deltopectoral incision. B. Axillary incision beginning inferior to the tip of the coracoid and progressing toward the anterior axillary fold. C. In this dissection, the subscapularis tendon is being tagged at the superior border of the rotator interval.
■ The location of the deltoid split depends on the pathology being managed. When the pathology requires more exposure, moving the deltoid split posteriorly will improve exposure (FIG 2B).
■ Subperiosteally, the anterior deltoid is elevated from the
acromion and the acromioclavicular joint. Continue the de- tachment by sharp dissection laterally to expose the anterior aspect of the acromion.
■ Bleeding will be encountered during this dissection as a result of the division of the acromial branch of the cora- coacromial artery.
■ The surgeon should not detach more of the deltoid than is necessary.
■ The deltoid split is extended 2 to 3 cm distal to the acromion.
■ Stay sutures are inserted in the apex of the split to prevent the muscle from inadvertently splitting distally during retraction and damaging the axillary nerve.
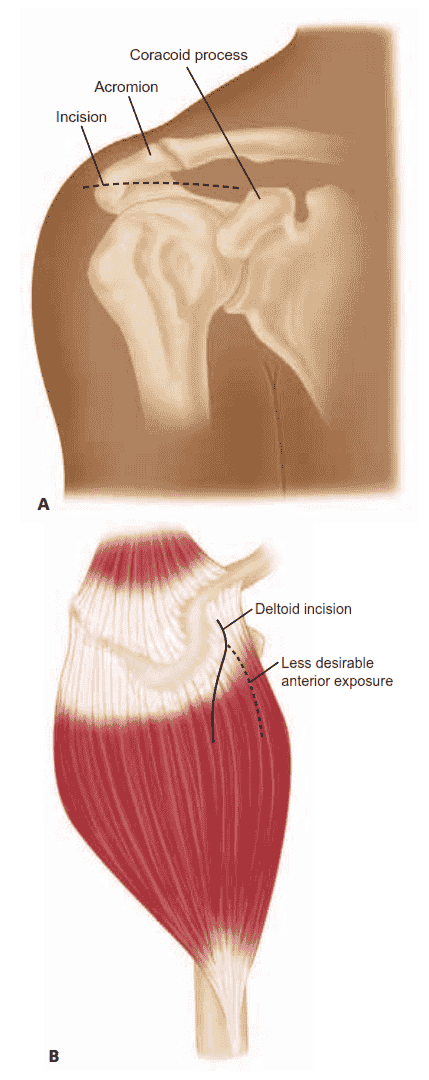
FIG 2 • A. Anterosuperior approach to the shoulder. A trans- verse incision begins at the anterolateral corner of the acromion and ends just lateral to the coracoid. B. The posterior curve of the deltoid incision can be moved more posteriorly, as depicted here, to allow necessary exposure as dictated by the pathology.
■ The split edges of the deltoid muscle are retracted to reveal the underlying coracoacromial ligament.
■ The coracoacromial ligament is detached from the acromion by sharp dissection.
■ The supraspinatus tendon with its overlying subacromial bursa now can be visualized.
■ The head of the humerus is rotated to expose different portions of the rotator cuff.
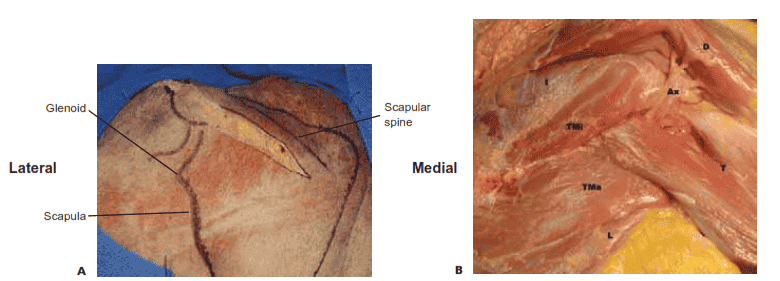
FIG 3 • A. Horizontal incision along the scapular spine allowing for the posterior approach to the shoulder. B. Cadaveric specimen de- picting the internervous plane between the infraspinatus and teres minor as well as the axillary nerve in the quadrangular space. (A: From Goss TP. Glenoid fractures: open reduction and internal fixation. In: Widd, DA, ed. Master Techniques in Orthopaedic Surgery: Fractures, ed 2. Philadelphia: Lippincott Williams & Wilkins, 1998:3–17; B: Courtesy of Jesse A. McCarron, MD, Michael Codsi, MD, and Joseph P. Iannotti, MD.)
POSTERIOR APPROACH TO THE SHOULDER
Indications
■ Repair in cases of recurrent posterior dislocation or sublux- ation of the shoulder
■ Glenoid osteotomy
■ Treatment of fractures of the scapular neck
■ Treatment of posterior fracture and dislocations of the proximal humerus
■ Spinoglenoid notch cyst drainage
Incision
■ A horizontal incision is made along the scapular spine ex- tending to the posterolateral corner of the acromion (FIG 3A)
Internervous Plane
■ Between teres minor (axillary nerve) and infraspinatus
(suprascapular nerve)
■ The suprascapular nerve passes around the base of the spine of the scapula as it runs from the supraspinatus fossa to the in- fraspinatus fossa.
Surgical Dissection
■ The origin of the deltoid is identified on the scapular spine. There are three ways to manage the deltoid during posterior exposures:
■ Detach the origin on the scapular spine
■ Split the deltoid muscle along the length of its fibers
■ Elevate the deltoid from the inferior margin
■ The plane between the deltoid muscle and the underlying in- fraspinatus muscle is identified.
■ The plane is easier to locate at the lateral end of the incision.
■ The internervous plane between the infraspinatus and teres minor muscles is identified (FIG 3B).
■ The axillary nerve runs longitudinally in the quadrangu-
lar space beneath the teres minor.
■ The posterior circumflex humeral artery runs with the ax- illary nerve in the quadrangular space between the inferior borders of the teres minor muscle.
■ The infraspinatus is retracted superiorly and the teres minor inferiorly to reach the posterior regions of the glenoid cavity and the neck of the scapula.
■ The posteroinferior corner of the shoulder joint capsule should be visible.
HUMERUS APPROACHES
ANTERIOR APPROACH TO THE HUMERUS
Indications
■ Internal fixation of fractures of the humerus
■ Management of humeral nonunions
■ Osteotomy of the humerus
Incision
■ A longitudinal incision is made over the tip of the coracoid process of the scapula; it runs distally and laterally in the line of the deltopectoral interval to the insertion of the deltoid muscle on the lateral aspect of the humerus, about halfway down its shaft.
■ The incision should be continued distally as far as necessary, following the lateral border of the biceps muscle (FIG 4A).
Internervous Plane
■ The anterior approach uses two different internervous planes.
■ Proximally, the plane lies between the deltoid muscle (supplied by axillary nerve) and the pectoralis major muscle (supplied by medial and lateral pectoral nerves) (FIG 4B).
■ Distally, the plane lies between the medial fibers of the
brachialis muscle (musculocutaneous nerve) and the lateral fibers of the brachialis muscle (radial nerve) (FIG 4C).
Surgical Dissection
Proximal Humeral Shaft
■ The deltopectoral interval is identified using the cephalic vein as a guide and the two muscles are separated, retracting the cephalic vein either medially with the pectoralis major or laterally with the deltoid.
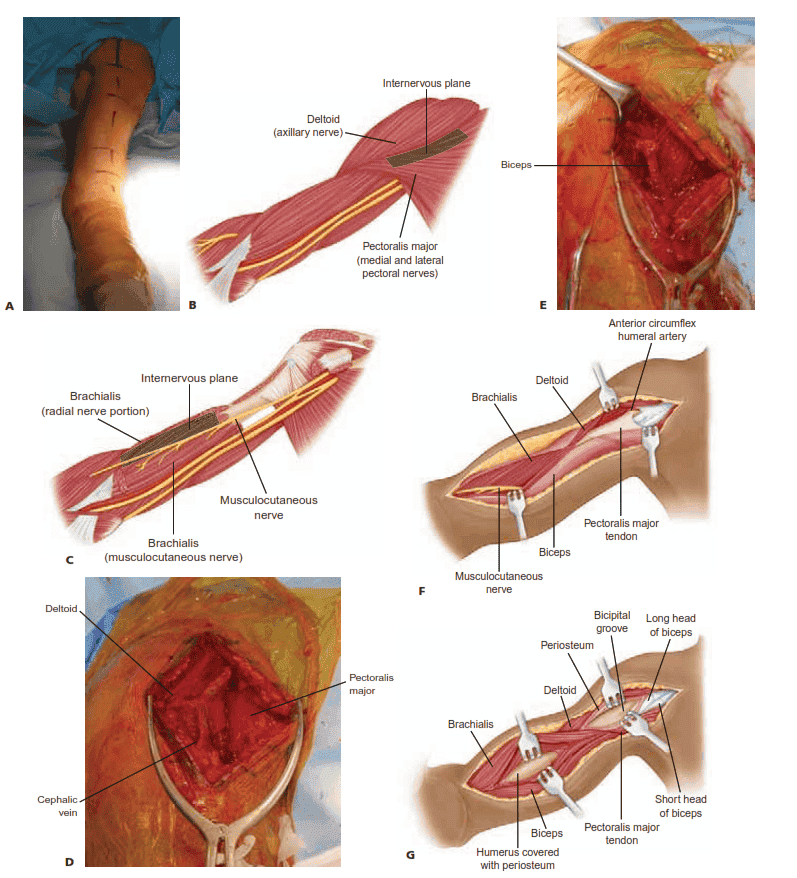
FIG 4 • A. Patient prepared for an anterior approach to the humerus. B. The internervous plane between the deltoid muscle and the pec- toralis major muscle. C. Further distally, one can appreciate the internervous plane between the medial fibers of the brachialis (musculocu- taneous nerve) medially and the lateral fibers of the brachialis (radial nerve) laterally. D. Deltopectoral incision: developing the interval between the deltoid and pectoralis major. The cephalic vein can be seen separating these two structures. E. With deeper dissection, the bi- ceps tendon is seen running in the rotator interval. F. Further distal dissection reveals the musculocutaneous nerve passing along the me- dial border of the biceps muscle. G. To expose the distal third of the humerus, the fibers of the brachialis are split. Flexion of the elbow
will relieve the tension off the brachialis, making the exposure easier. (A: Courtesy of Matthew J. Garberina, MD, and Charles L. Getz, MD.)
■ The muscular interval is developed distally down to the in- sertion of the deltoid into the deltoid tuberosity and the inser- tion of the pectoralis major into the lateral lip of the bicipital groove (FIG 4D,E).
■ To expose the bone fully, the surgeon may need to detach
part or all of the insertion of pectoralis major muscle.
■ The minimum amount of soft tissue should be detached to allow adequate visualization and reduction of the fracture.
■ If further exposure is needed, the surgeon dissects medially in a subperiosteal manner to avoid damage to the radial nerve, which lies in the spiral groove of the humerus and crosses the back of the middle third of the bone in a medial to lateral direction.
Distal Humeral Shaft
■ The surgeon identifies the muscular interval between the bi- ceps brachii and brachialis.
■ The interval is developed by retracting the biceps medially
(FIG 4F).
■ Beneath it lies the brachialis muscle, which covers the humeral shaft.
■ The fibers of the brachialis are split longitudinally in the in- terval between the medial 2/3 and the lateral 1/3 to expose the periosteum on the anterior surface of the humeral shaft.
■ The periosteum is incised longitudinally in line with the muscle dissection, and the brachialis is stripped off the ante- rior surface of the bone (FIG 4G).
■ In the anterior compartment of the distal third of the arm,
the radial nerve pierces the lateral intermuscular septum and lies between the brachioradialis and brachialis muscles.
POSTERIOR APPROACH TO THE HUMERUS
Indications
■ Open reduction and internal fixation of a fracture of the humerus
■ Treatment of nonunion
■ Exploration of the radial nerve in the spiral groove
Incision
■ A longitudinal incision is made in the midline of the poste- rior aspect of the arm, from 8 cm below the acromion to the olecranon fossa (FIG 5A).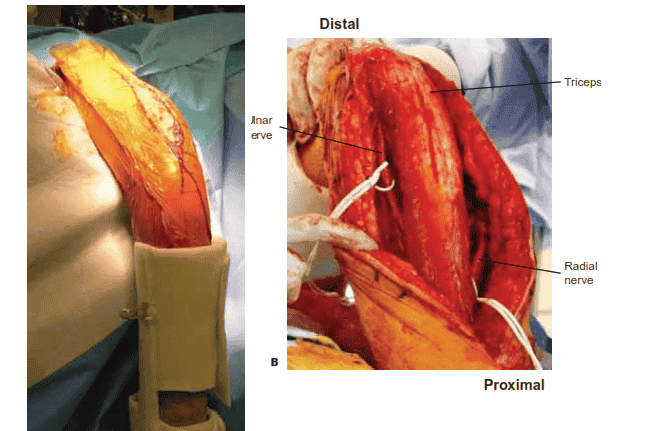
Internervous Plane
■ There is no true internervous plane; dissection involves sep- arating the heads of the triceps brachii muscles, all of which are supplied by the radial nerve.
■ The medial head, which is the deepest, has a dual nerve sup- ply (radial and ulnar nerves).
Surgical Dissection
■ The surgeon incises the deep fascia of the arm in line with the skin incision.
■ The triceps muscle has two layers:
■ The outer layer consists of two heads: the lateral head arises from the lateral lip of the spiral groove, and the long head arises from the infraglenoid tubercle of the scapula (FIG 5B).
■ The inner layer consists of the medial head, which arises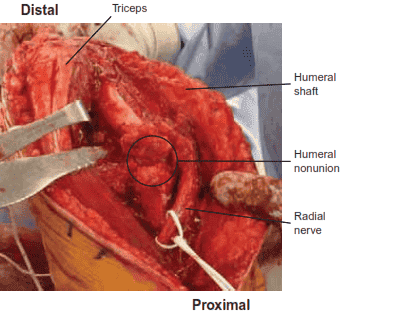
FIG 5 • (continued) C. In this humeral shaft nonunion, the tri- ceps is reflected medially and the radial nerve can be seen passing through the spiral groove. (A: Courtesy of Matthew J. Garberina, MD, and Charles L. Getz, MD.)
below the spiral groove all the way down to the distal fourth
of the bone. A
■ The spiral groove contains the radial nerve; the radial
nerve separates the origins of the lateral and medial heads
(FIG 5C).
■ To avoid iatrogenic nerve injury, the surgeon should never continue dissection down to bone in the proximal two thirds of the arm until the radial nerve has been identified.
MODIFIED POSTERIOR APPROACH TO THE HUMERUS
Indications
■ Open reduction and internal fixation of humeral shaft fractures
■ Open reduction and internal fixation of lateral condyle fractures
■ Treatment of humeral nonunion
■ Exploration of the radial nerve in the spiral groove
Incision
■ The surgeon makes a straight incision along a line between the posterolateral aspect of the acromion and the lateral edge of the olecranon.
■ The length of the incision is dictated by the requirement for exposure.
■ Extensile exposure is limited proximally by the axillary nerve.
Internervous Plane
■ There is no true internervous plane, because both the medial B
Lower lateral brachial cutaneous nerve
Continuation of radial nerve to forearm, piercing intermuscular septum
and lateral heads of the triceps are supplied by the radial nerve.
Surgical Dissection
■ The deep fascia is incised in line with the skin incision along the lateral aspect of the triceps.
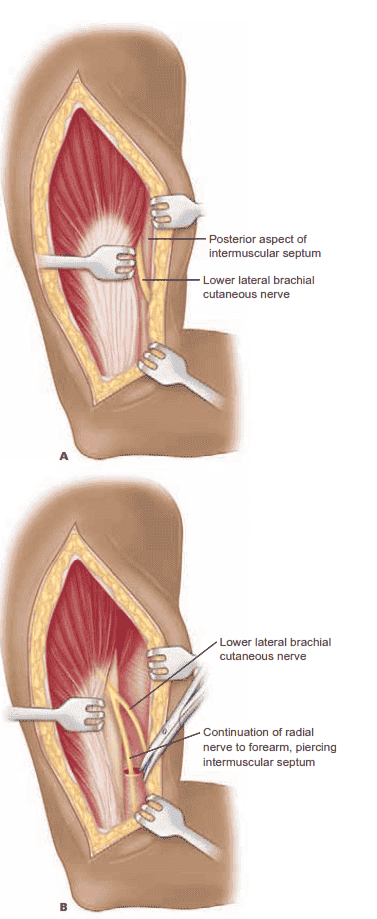 FIG 6 • A. The lower lateral brachial cutaneous nerve, which branches off the radial nerve, is identified along the posterior aspect of the intermuscular septum. The entire triceps here is retracted slightly medially. B. The intermuscular septum is di- vided deep to the lower lateral brachial cutaneous nerve for
FIG 6 • A. The lower lateral brachial cutaneous nerve, which branches off the radial nerve, is identified along the posterior aspect of the intermuscular septum. The entire triceps here is retracted slightly medially. B. The intermuscular septum is di- vided deep to the lower lateral brachial cutaneous nerve for
3 cm to expose the radial nerve distally. (continued)
■ Triceps preserving
■ Olecranon osteotomy
Lateral head of triceps
Medial head of triceps
C
Axillary nerve
Branch to medial head of triceps
Lower lateral brachial cutaneous nerve
Open region of intermuscular septum
Triceps-Splitting Approaches
Posterior Triceps-Splitting Approach (Campbell)
■ Care must be exercised to maintain the medial portion of the triceps expansion over the forearm fascia in continuity with the flexor carpi ulnaris.
■ Laterally, the anconeus and triceps are more stable, with less chance of disruption.
INDICATIONS
■ Total elbow arthroplasty
■ Distal humerus fracture
■ Removal of loose bodies
■ Capsulectomies
■ Posterior exposure of the joint for ankylosis, sepsis, syn- ovectomy, and ulnohumeral arthroplasty
APPROACH
■ Skin incision begins in the midline over the triceps, about
10 cm above the joint line, and is generally placed laterally or medially across the tip of the olecranon. It continues distally over the lateral aspect of the subcutaneous border of the proximal ulna for about 5 to 6 cm (FIG 7A).
■ Triceps is exposed, along with the proximal 4 cm of the ulna.
■ A midline incision is made through the triceps fascia and tendon as it is continued distally across the insertion of the
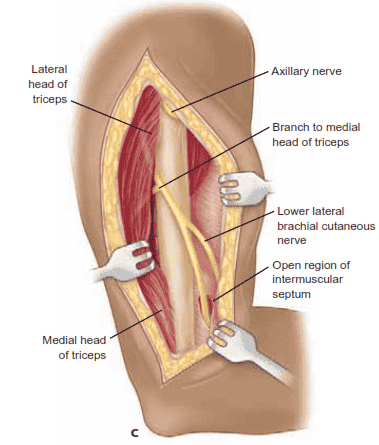 FIG 6 • (continued) C. The medial and lateral heads of the
FIG 6 • (continued) C. The medial and lateral heads of the
triceps are retracted subperiosteally in a medial direction to expose the posterior aspect of the humeral diaphysis.
■ The triceps is retracted medially and the lower lateral brachial cutaneous nerve branch from the radial nerve is iden- tified. This nerve is traced proximally to the main trunk of the radial nerve (FIG 6A).
■ The intermuscular septum is divided distally to allow the ra-
dial nerve to be mobilized (FIG 6B).
■ Subperiosteally, the medial and lateral heads of the triceps are reflected medially to expose the humeral shaft (FIG 6C).
ELBOW APPROACHES
■