ELBOW Surgical Approaches
ELBOW APPROACHES
■ The surgical exposures described for the elbow are divided into posterior, medial, and lateral approaches. These descrip- tions denote the deep surgical interval employed.
■ Often, these deep approaches can be performed through a direct medial or lateral skin incision or a more versatile poste- rior incision.
POSTERIOR APPROACH TO THE ELBOW
■ Releasing the triceps attachment to the olecranon is not advisable, owing to the difficulty of adequate repair and possible disruption during rehabilitation. Today, there are four choices of posterior exposure:
■ Triceps splitting
■ Triceps reflecting
triceps tendon at the tip of the olecranon and down the sub- cutaneous crest of the ulna (FIG 7B).
■ Triceps tendon and muscle are split longitudinally, exposing the distal humerus.
■ Anconeus is then reflected subperiosteally laterally, while the flexor carpi ulnaris is similarly retracted medially.
■ Insertion of the triceps is carefully released from the olecranon, leaving the extensor mechanism in continuity with the forearm fascia and muscles medially and laterally (FIG 7C).
■ Ulnar nerve is visualized and protected in the cubital tunnel
■ Closure of the triceps fascia is required only proximal to the olecranon, but the insertion should be repaired to the ole- cranon with a suture passed through the ulna.
■ The incision is then closed in layers.
Triceps-Splitting, Tendon-Reflecting Approach (Van Gorder)
■ A variation of the technique described earlier
■ Allows lengthening of the triceps if necessary
■ Has been largely abandoned in favor of the triceps-reflecting techniques
INDICATIONS
■ Same as those for midline-splitting approach described earlier
APPROACH
■ A posterior midline incision begins 10 cm proximal to the olecranon and extends distally onto the subcutaneous border of the ulna between the anconeus and the flexor carpi ulnaris.
■ Triceps fascia and aponeurosis are exposed along the tendi- nous insertion into the ulna.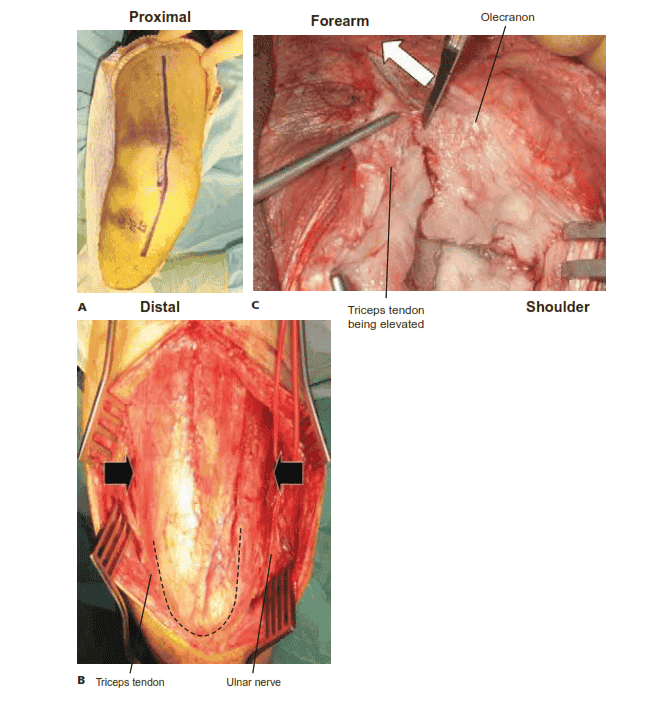
FIG 7 • A. Skin incision for the posterior triceps- splitting approach. B. Medial and lateral flaps are elevated, allowing full access to the triceps ten- don. The ulnar nerve is isolated along the medial border with a vessel loop. C. The insertion of the triceps being elevated off the olecranon from me- dial to lateral. (A: Courtesy of Asif M. Ilyas, MD, and Jesse B. Jupiter, MD; B,C: Courtesy of Srinath Kamineni, MD.)
■ Tendon is reflected from the muscle in a proximal to distal direction, freeing the underlying muscle fibers while preserving the tendinous attachment to the olecranon (FIG 8).
■ Triceps muscle is then split in midline, and the distal
humerus is exposed subperiosteally.
■ Periosteum and triceps are elevated for a distance of about
5 cm proximal to the olecranon fossa, exposing the posterior aspect of the joint.
■ If more extensive exposure is desired, the subperiosteal dis- section is extended to the level of the joint, exposing the condyles both medially and laterally.
■ Ulnar nerve should be identified and protected.
■ After the procedure, if an elbow contracture has been cor- rected, the joint should be maximally flexed.
■ The tendon slides distally from its initial position, and the proximal muscle and tendon are reapproximated in the length- ened relationship.
■ The distal part of the triceps is then securely sutured to the fascia of the triceps expansion, and the remainder of the wound is closed in layers.
Triceps-Reflecting Approaches
■ The triceps mechanism may be preserved in continuity with the anconeus and simply reflected to one side or the other.
■ Three surgical approaches have been described that preserve the triceps muscle and tendon in continuity with the distal musculature of the forearm fascia and expose the entire joint.
Bryan-Morrey Posteromedial Triceps-Reflecting Approach
■ Developed to preserve the continuity of the triceps with the anconeus
INDICATIONS
■ Total elbow arthroplasty
■ Interposition arthroplasty
FIG 8 • Triceps-splitting, tendon-reflecting approach. The tendon is reflected from the muscle in a proximal to distal direction.
Triceps attachment
Ulnar periosteum
Ulnar nerve translocated
■ Elbow dislocation
■ Distal humerus fracture
■ Synovial disease
■ Infection
APPROACH
■ A straight posterior incision is made medial to the midline, about 9 cm proximal and 8 cm distal to the tip of the olecra- non (FIG 9A).
■ The ulnar nerve is identified proximally at the margin of the
medial head of the triceps and, depending on the procedure, is either protected or carefully dissected to its first motor branch and transposed anteriorly.
■ The medial aspect of the triceps is elevated from the poste- rior capsule.
■ The fascia of the forearm between the anconeus and the flexor carpi ulnaris is incised distally for about 6 cm.
■ The triceps and the anconeus are elevated as one flap from medial to lateral, skeletonizing the olecranon and subcuta- neous border of the ulna (FIG 9B). This should be performed at 20 to 30 degrees of flexion to relieve tension on the inser-
tion, thereby facilitating dissection.
B
Lateral capsule
C
Radial head
Anconeus
■ The collateral ligaments may be released from the humerus for exposure as needed (FIG 9C).
■ If stability is important, these ligaments should be pre-
served or anatomically repaired at the conclusion of the surgery.
■ When performing a linked total elbow replacement, it is not necessary to preserve or repair the collateral ligaments.
FIG 9 • The Bryan-Morrey posterior approach. A. Straight
posterior skin incision. B. The ulnar nerve has been translo- cated anteriorly. The medial border of the triceps is identified and released and the superficial forearm fascia is sharply incised to allow reflection of the fascia and perios-
teum from the proximal ulna. C. The extensor mechanism has
been reflected laterally and the collateral ligaments have been released.
Chapter 2 SURGICAL APPROACHES TO THE SHOULDER AND ELBOW 3065
■ The triceps attachment can be thin at the attachment to the ulna and it is not uncommon for a buttonhole to be created when reflecting the triceps.
■ To prevent this, the flap can be raised as an osteope- riosteal flap (see osteocutaneous flap approach).
■ A small osteotome is used to elevate the fascia with the petals of bone.
■ The flap is mobilized laterally, elevating the anconeus ori- gin from the distal humerus until it can be folded over the lateral humeral condyle.
■ At this point, the radial head can be visualized.
■ The tip of the olecranon can be excised to help expose the trochlea.
Osteoanconeus Flap Approach
■ This provides excellent extension and reliable healing of the osseous attachment to the olecranon.
■ This approach exposes only the ulnar nerve, whereas the
Mayo approach translocates the nerve.
INDICATIONS
■ This is a triceps-reflecting approach similar in concept to the
Bryan-Morrey triceps-reflecting approach.
■ Most often used for joint replacement or distal humeral fractures
■ Proximally, the triceps is identified and freed from the bra- chioradialis and extensor carpi radialis longus along the intra- muscular septum to the level of the joint capsule.
■ The interval between the extensor carpi ulnaris and the an- coneus is identified distally.
■ The triceps in continuity with the anconeus is subpe- riosteally reflected. Sharp dissection frees the bony attach- ment of the triceps expansion to the anconeus from the lateral epicondyle.
■ The triceps remains attached to the tip of the olecranon.
■ The lateral collateral ligament complex is released from the humerus.
■ The joint may be dislocated with varus stress. If additional exposure is necessary, the anterior and posterior capsule can be released.
■ Routine closure of layers is performed, but the radial collat- eral ligament should be reattached to the bone through holes placed in the lateral epicondyle.
APPROACH
■ A straight posterior incision is made medial to the midline, about 9 cm proximal and 8 cm distal to the tip of the olecranon.
■ The ulnar nerve is identified and protected, but not translocated.
■ The triceps attachment is released from the ulna by os- teotomizing the attachment with a thin wafer of bone.
■ This is the essential difference from the Bryan-Morrey approach.
■ The medial aspect of the triceps, in continuity with the an- coneus, is elevated from the ulna (FIG 10A,B).
■ The collateral ligaments are either maintained or released,
depending on the pathology being addressed and the need for stability.
■ After the surgical procedure, the wafer of bone is secured to its bed by nonabsorbable sutures placed through bone holes (FIG 10C).
■ Interrupted sutures are used to repair the remaining distal
portion of the extensor mechanism.
Extensile Kocher Posterolateral Triceps-Reflecting Approach
Ulnar nerve
Osteotomy
Triceps brachii
INDICATIONS
■ Joint arthroplasty
■ Ankylosis
■ Distal humerus fractures
■ Synovectomy
■ Radial head excision
■ Infection
Flexor carpi ulnaris
Anconeus
APPROACH
■ Extensile exposure from the Kocher approach
■ Skin incision begins 8 cm proximal to the joint just posterior to the supracondylar ridge and continues distally over the Kocher interval between the anconeus and extensor carpi ul- naris about 6 cm distal to the tip of the olecranon

FIG 10 • Posterior view of the right elbow demonstrates a straight fascial incision to the lateral aspect of the tip of the olecranon. A. The line of release after the ulnar nerve has been identified and protected. (continued)
3066
Triceps brachii reflected with capsule
Annular ligament
Olecranon cap
Anconeus
B
FIG 10 • (continued) B. The olecranon has been os- teotomized and the triceps swept from medial to lat- eral in continuity with the anconeus and forearm fas- cia. C. Closure with sutures placed through bone and the distal extensor mechanism is done with interrupted
sutures. C
Mayo Modified Extensile Kocher Approach
■ The extensile Kocher approach and the Mayo modification of the extensile Kocher approach provide sequentially greater exposure from the initial Kocher approach.
INDICATIONS
■ Release of ankylosed joint
■ Interposition arthroplasty
■ Replacement arthroplasty
APPROACH
■ A modification of the extensile Kocher approach consists of reflecting the anconeus and triceps expansion from the tip of the olecranon by sharp dissection.
■ The extensor mechanism (triceps in continuity with the an- coneus) may be reflected from lateral to medial.
■ The ulnar nerve should be decompressed or transposed if an extensile lateral approach is used.
■ The triceps is reattached in a fashion identical to that de- scribed for the Mayo approach.
Triceps-Preserving Approaches
Posterior Triceps-Sparing Approach
■ Because the triceps is not elevated from the tip of the olecra- non, rapid rehabilitation is possible.
INDICATIONS
■ Tumor resection
■ Joint reconstruction for resection of humeral nonunion
■ Joint replacement
APPROACH
■ A posterior incision is made medial to the tip of the olecranon.
■ Medial and lateral subcutaneous skin flaps are elevated.
■ The ulnar nerve is identified and transposed anteriorly.
■ The medial and lateral aspects of the triceps are identified and developed distally to the triceps attachment on the ulna.
■ For distal humerus fractures fixation:
■ The common flexors and common extensors are partially released from the distal humerus to expose the supracondy- lar column for plate fixation.
■ For total elbow arthroplasty or tumor resection:
■ The common flexors and extensors are fully released from the medial and lateral epicondyle. The collateral ligaments and capsule are released and the distal humerus is excised.
■ The distal humerus is exposed by bringing it through the defect along the lateral margin of the triceps.
■ The ulna is exposed by supinating the forearm.
■ After the implant has been inserted, the joint is articulated.
Chapter 2 SURGICAL APPROACHES TO THE SHOULDER AND ELBOW 3067
■ There is no need to close or repair the extensor mechanism with this approach.
Olecranon Osteotomy
■ Worldwide, the transosseous approach is probably the ex- posure most often used, especially for distal humeral fractures. The oblique osteotomy has almost been abandoned, and the transverse osteotomy has largely been replaced by the chevron.
Chevron Transolecranon Osteotomy
■ Intra-articular osteotomy, first described by MacAusland, was originally recommended for ankylosed joints.
■ It has been adapted by some for radial head excision and synovectomy and used or modified by others for T and Y condylar fractures.
■ The chevron osteotomy enhances rotational stability com- pared to a transverse osteotomy.
INDICATIONS
■ Ankylosed joints
■ T or Y condylar fractures
APPROACH
■ A posterior incision is made medial to the tip of the olecranon.
■ Medial and lateral subcutaneous skin flaps are elevated.
■ The ulnar nerve is identified and transposed anteriorly.
■ The medial and lateral aspects of the triceps are identified and developed distally to the triceps attachment on the ulna.
■ An apex-distal chevron or V osteotomy is performed with a thin oscillating saw but not completed through the subchondral bone. An osteotome completes the osteotomy, creating irregular surfaces that interdigitate increasing stability (FIG 11A,B).
■ The triceps tendon, along with the osteotomized portion of
the olecranon, may then be retracted proximally, and by flex- ing the elbow joint, the joint can be exposed (FIG 11C).
■ Occasionally the medial or lateral collateral ligaments are released for better exposure.
■ These ligaments are then repaired at the end of the procedure.
■ At the completion of the procedure, the tip of the olecranon is secured via tension-band or plate fixation.
LATERAL APPROACH TO THE ELBOW
■ Lateral exposures to the elbow are widely used to treat a va- riety of elbow pathologies. The exposures differ according to the deep interval used.
■ With any of the lateral exposures to the joint or to the proximal radius, the surgeon must be constantly aware of the possibility of injury to the posterior interosseous or recurrent branch of the radial nerve.
Anterolateral Approach to the Elbow (Kaplan)
Indications
■ Anterior capsular release
■ Posterior interosseous nerve exposure
■ Capitellar/lateral column fractures
Approach
■ Deep interval for the anterolateral approach lies between the extensor digitorum communis and the extensor carpi radialis longus muscles. (Intermuscular interval is best found by ob- serving where vessels penetrate the fascia along the anterior margin of the extensor digitorum communis aponeurosis.)
■ Fascia is split longitudinally between the extensor digito- rum communis and the extensor carpi radialis longus. (As the dissection is carried deep through the extensor carpi radialis longus, the extensor carpi radialis brevis is encountered.)
■ Deep to the extensor carpi radialis brevis, the transversely oriented fibers of the supinator are encountered, along with the posterior interosseous nerve. The posterior interosseous
Triceps
Ulnar nerve
Distal humerus
A B C
FIG 11 • Olecranon osteotomy. A. The triceps is released medially and laterally, while the ulnar nerve is protected. B. A chevron os- teotomy with a distal apex is initiated with an oscillating saw. C. The proximal portion containing the olecranon osteotomy and tri- ceps tendon is retracted proximally, exposing the elbow joint.
3068
nerve defines the distal extent of the exposure. Pronation moves the radial nerve away from the surgical field.
■ If required, proximal dissection with elevation of the ex- tensor carpi radialis longus, extensor carpi radialis brevis, and brachioradialis anteriorly from the lateral supracondy- lar ridge of the humerus provides exposure of the anterior joint capsule.
Modified Distal Kocher Approach
Indications
■ Reconstruction of the lateral ulnar collateral ligament
Approach
■ The skin incision begins just proximal to the lateral epi- condyle of the humerus and extends obliquely for about 6 cm in line with the fascia of the anconeus and extensor carpi ul- naris muscles (FIG 12A).
■ The Kocher interval between the anconeus and flexor carpi
ulnaris is incised (FIG 12B).
■ Development of the Kocher interval reveals the lateral joint capsule.
■ The anconeus is then reflected posteriorly off the joint cap- sule distally to expose the crista supinatoris.
■ The extensor carpi ulnaris and the common extensor tendon are released from the lateral epicondyle and reflected anteriorly, exposing the lateral capsule. The radial nerve is at a safe distance from the dissection, and it is protected by the extensor carpi ul- naris and extensor digitorum communis muscle mass (FIG 12C).
■ A longitudinal incision is made through the capsules to ex-
pose the radiocapitellar joint.
Boyd (Posterolateral) Approach
■ Radioulnar synostosis may occur as the proximal radius and ulna are exposed subperiosteally.
Indications
■ Monteggia fracture-dislocations
■ Radial head fractures
■ Radioulnar synostosis
Approach
■ The incision begins just posterior to the lateral epicondyle lateral to the triceps tendon and continues distally to the lat-
Triceps
Incision
Incision
Lateral epicondyle
Anconeus
Extensor carpi ulnaris
B
Triceps
A
Anconeus
Lateral epicondyle
FIG 12 • Distal Kocher approach.
A. The incision begins about 2 to 3 cm above the lateral epicondyle over the supracondylar ridge and extends dis- tally and posteriorly for about 4 cm.
B. The interval between the anconeus
and the extensor carpi ulnaris is iden- tified. C. Development of this interval reveals the capsule.
Incision in
C capsule
Extensor carpi ulnaris
Chapter 2 SURGICAL APPROACHES TO THE SHOULDER AND ELBOW 3069
eral tip of the olecranon and then down to the subcutaneous border of the ulna.
■ The anconeus and supinator are subperiosteally elevated from the subcutaneous border of the ulna (anconeus and supinator) (FIG 13A,B).
■ Retraction of the anconeus and supinator exposes the joint
capsule overlying the radial head and neck.
■ The supinator muscle protects the posterior interosseous nerve.
■ This lateral capsule contains the lateral ulnar collateral lig- ament, and its division can lead to posterolateral rotatory instability.
■ To expose the radial shaft, the incision may be continued along the subcutaneous ulnar border, elevating the muscles off the lateral aspect of the ulna (extensor carpi ulnaris, abductor pollicis longus, and extensor pollicis longus).
■ The posterior interosseous and recurrent interosseous arter- ies may need ligation.
MEDIAL APPROACH TO THE ELBOW
■ There are relatively few indications for medial exposure of the elbow joint. This has been superseded by arthroscopic approaches.
■ The most valuable contribution to medial joint exposure is that described by Hotchkiss. This extensile exposure provides greater flexibility, particularly for exposure of the coronoid and for contracture release.
Extensile Medial Over-the-Top Approach
■ Excellent visualization of the anteromedial and postero- medial elbow
■ Not a sufficient approach for excision of heterotopic bone on the lateral side of the joint
■ Does not provide adequate access to the radial head
Indications
■ Coronoid fractures
■ Contracture release (when ulnar nerve exploration required)
■ Anterior and posterior access to the joint
Line of incision
Anconeus
Triceps tendon
Olecranon
A
Flexor carpi ulnaris
Extensor carpi ulnaris
Flexor digitorum profundus
■ May be converted to a triceps-reflecting exposure of Bryan- Morrey
Approach
■ Superficial dissection
■ Skin incision can vary between the boundaries of a pure posterior skin incision and midline medial incision (FIG 14A).
■ Subcutaneous skin is elevated.
■ The medial supracondylar ridge of the humerus, the me- dial intramuscular septum, the origin of the flexor pronator mass, and the ulnar nerve are identified.
■ Anterior to the septum, running just on top of the fascia (not in the subdermal tissue), the medial antebrachial cuta- neous nerve is identified and protected.
■ The ulnar nerve is identified. If the patient previously had
Reflected anconeus
Reflected portion of supinator from ulna
Divided portion of supinator
surgery, the ulnar nerve should be identified proximally be-
fore the surgeon proceeds distally.
■ If anterior transposition was performed previously, the nerve should be mobilized carefully before the operation proceeds.
■ The surface of the flexor pronator muscle mass origin is found by sweeping the subcutaneous tissue laterally with the medial antebrachial cutaneous nerve in this flap of subcuta- neous tissue.
■ The medial intramuscular septum divides the anterior and posterior compartments of the elbow. The medial intramus- cular septum is ultimately excised from the medial epi- condyle to 5 cm proximal to it (FIG 14B).
■ The ulnar nerve is protected and the veins at the base of
the septum are cauterized.
Reflected portion of
B supinator from radius
FIG 13 • The Boyd approach. A. The incision begins along the lateral border of the triceps about 2 to 3 cm above the epi- condyle and extends distally over the lateral subcutaneous bor- der of the ulna about 6 to 8 cm past the tip of the olecranon. The ulnar insertion of the anconeus and the origin of the supinator muscle are elevated subperiosteally. More distally, the subperiosteal reflection includes the abductor pollicis longus,
the extensor carpi ulnaris, and the extensor pollicis longus mus- cles. The origin of the supinator at the crista supinatorus of the ulna is released, and the entire muscle flap is retracted radially, exposing the radiohumeral joint. B. The posterior interosseous nerve is protected in the substance of the supinator.
■ Deep anterior exposure
■ The flexor pronator mass origin is identified and totally or partially released from the medial epicondyle.
■ If extensile exposure is needed, the entire flexor pronator mass is elevated from the medial epicondyle (FIG 14C,D).
■ If less extensile exposure is needed, the flexor pronator
mass is divided parallel to the fibers, leaving about 1.5 cm of flexor carpi ulnaris tendon attached to the epicondyle.
■ A small cuff of fibrous tissue of the origin can be left on the supracondylar ridge as the muscle is elevated; this fa- cilitates reattachment when closing.
■ The flexor pronator origin should be dissected down to the level of bone but superficial to the joint capsule. As this
3070
plane is developed, the brachialis muscle is encountered from the underside.
■ The brachialis muscle is identified along the supracondylar ridge and released in continuity with the flexor pronator mass.
■ These muscles should be kept anterior and elevated from the capsule and anterior surface of the distal humerus.
■ The median nerve and the brachial vein and artery are su- perficial to the brachialis muscle and protected with the sub- periosteal release of the brachialis.
■ Dissection of the capsule proceeds laterally and distally to separate it from the brachialis.
■ In the case of contracture, the capsule, once separated from the overlying brachialis and brachioradialis, can be sharply excised (FIG 14E).
■ Deep posterior capsule exposure
■ The ulnar nerve is mobilized to permit anterior transposi- tion with a dissection carried distally to the first motor branch to allow the nerve to rest in the anterior position without being sharply angled as it enters the flexor carpi ulnaris.
■ With the Cobb elevator, the triceps is elevated from the posterior distal surface of the humerus.
■ The posterior capsule can be separated from the triceps as the elevator sweeps from the proximal to distal.
■ Closure
■ The flexor pronator mass should be reattached to the supracondylar ridge.
■ The ulnar nerve should be transposed and secured with a fascial sling to prevent posterior subluxation.
A B
C D
FIG 14 • A. Medial skin incision along the midline.
B. The medial intermuscular septum (light blue) is ex- cised from the medial epicondyle to 5 cm proximal to it. The ulnar nerve is shown tagged with a suture loop.
C,D. If the extensile exposure is needed, the entire flexor
pronator muscle mass is elevated from the medial epi- condyle. E. The capsule can be sharply excised in cases of
E capsular contracture.