
Applied Surgical Anatomy of the Posterior Approach to the Knee
Overview
The anatomy of the posterior approach to the knee is the anatomy of the popliteal fossa.
The popliteal fossa is diamond-shaped in cadavers. In live patients, the lower "V" of the diamond (the gap between the two heads of the gastrocnemius muscle) is nonexistent until the heads are retracted from one another.
The fossa is bounded on its superior border by the semimembranosus and semitendinosus muscles medially and by the biceps femoris muscle laterally. Its inferior boundaries are the two heads of the gastrocnemius muscle. The roof of the fossa is the popliteal fascia, which is formed by the outer layer of the knee's supporting structures. The floor is the posterior aspect of the distal end of the femur, the posterior capsule of the joint, and the popliteus muscle, which overlies the proximal tibia.
Incision
The lines of cleavage in the skin run almost transversely across the back of the knee joint. The curved incision described, therefore, has a variable relation to these lines. The resultant scar usually is cosmetically acceptable.
The incision crosses a major flexor crease at the back of the knee, but because the incision is almost parallel to the skin crease at this level, a flexion contracture of the knee does not occur when the wound heals.
Superficial Surgical Dissection
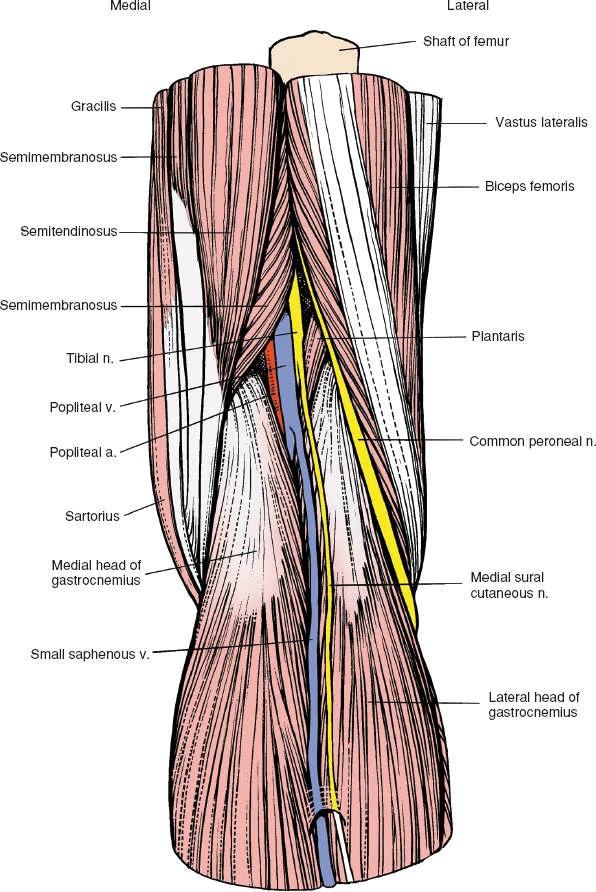
Superficial surgical dissection involves incising the roof of the popliteal fossa, using the small (short) saphenous vein and the medial sural cutaneous nerve of the calf as guides.
The roof of the popliteal fossa consists of the popliteal fascia, a continuation of the deep fascia of the thigh, and part of the outer layer of the knee. Two key structures pierce it to form the basis for the dissection of the fossa itself:
- The small (short) saphenous vein arises in the foot and runs behind the lateral malleolus into the back of the calf. It travels roughly along the midline of the calf and penetrates the popliteal fascia before joining the popliteal vein.
- The medial sural cutaneous nerve also runs in the midline of the calf beneath the deep fascia, just lateral to the small saphenous vein. This nerve, which is a branch of the tibial nerve, supplies varying amounts of skin on the back of the calf.
Knowing the location of these two structures makes it easier to find the tibial nerve.
The tibial nerve, a continuation of the sciatic nerve, is lateral to the popliteal artery as it enters the popliteal fossa. Then, at the midpoint of the fossa, it crosses the artery and lies medial to it as they leave the fossa together. The tibial nerve passes vertically downward in the fossa, giving branches to the plantaris, gastrocnemius, soleus, and popliteus muscles. Its sole cutaneous branch, the sural nerve, is of surgical interest in nerve grafting. The tibial nerve leaves the fossa between the two heads of the gastrocnemius muscle. Tibial nerve palsy affects the plantar flexors of the toes and ankle.
The common peroneal nerve slopes downward across the fossa, running laterally toward the medial side of the tendon of the biceps muscle. It disappears into the peroneus longus muscle, usually under a fibrous arch, where it may be entrapped before it winds around the fibula. Because patients naturally lie with their legs externally rotated, the head of the fibula often is in contact with the bed and compression palsy of the nerve can occur. For this reason, it is critically important to pad the head of the fibula when the patient is placed on the operating table in such a position that the head of this bone may come in contact with the operating table surface. Its division into deep and superficial peroneal nerves occurs within the substance of the peroneus longus muscle. Common peroneal nerve palsy affects all the extensors and evertors of the foot.
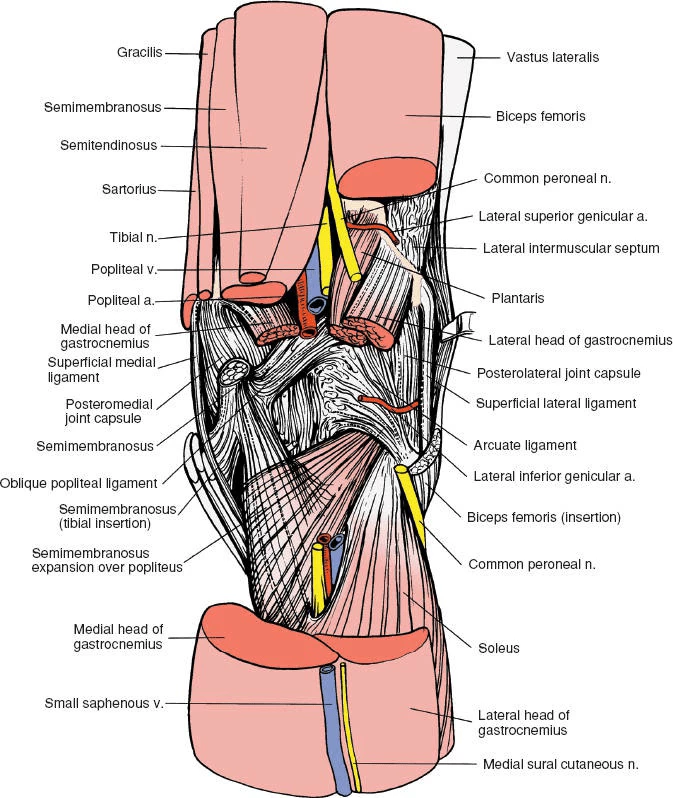
The vascular structures lie more deeply in the fossa. The popliteal artery runs obliquely through the fossa after entering on the medial side of the femur. It lies directly behind the posterior capsule of the knee joint, dividing into its terminal branches, the posterior tibial, anterior tibial, and peroneal arteries, behind the gastrocnemius muscle. In the fossa, it gives off five branches.
The two superior genicular arteries encircle the lower end of the femur. The lateral artery requires ligation in the posterolateral approach to the knee. The medial artery requires ligation if the medial head of the gastrocnemius muscle has to be detached from the femur to expose the posteromedial corner of the knee.
The middle genicular artery passes forward in the knee and supplies the cruciate ligaments. Traumatic rupture of the cruciate ligaments, therefore, is associated with brisk intra-articular bleeding that usually manifests as an immediate posttraumatic effusion. The artery holds its parent trunk firmly to the posterior capsule of the joint. For this reason, it can be damaged easily in dislocations of the knee during trauma or surgery. It also may be damaged as the posterior structures in the knee are dissected out from medial or lateral approaches. To avoid endangering the artery, flex the knee to allow the joint capsule to fall away from the back of the femur and tibia.
The two inferior genicular arteries (medial and lateral) encircle the upper end of the tibia, passing deep to the medial and lateral superficial ligaments. The lateral artery is the most commonly damaged structure during lateral meniscectomy; it runs right at the level of the joint line and, therefore, is vulnerable in cases in which the meniscus is detached too far laterally.
Deep Surgical Dissection and Its Dangers
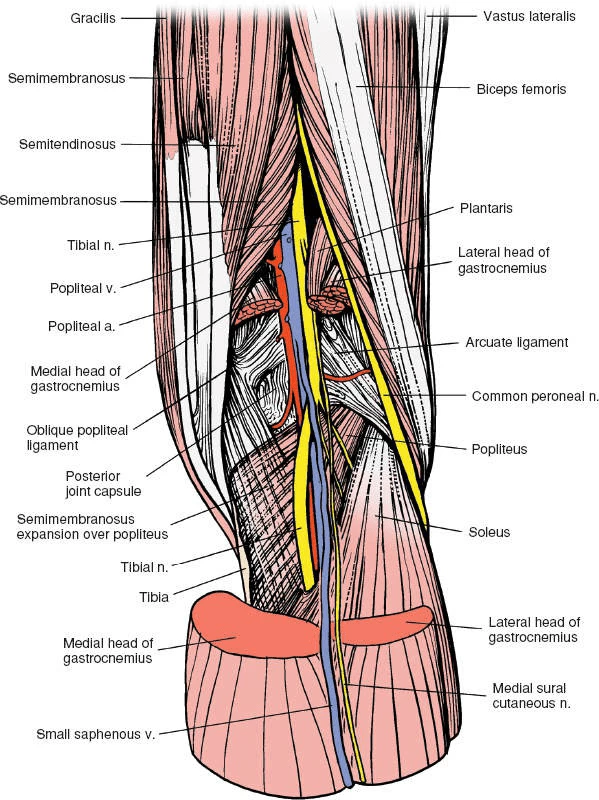
Deep surgical dissection consists of retracting and, sometimes, mobilizing the boundaries of the popliteal fossa. These boundaries are formed by the semimembranosus and semitendinosus muscles superomedially, by the biceps femoris muscle superolaterally, by the medial head of the gastrocnemius muscle inferomedially, and by the lateral head of the gastrocnemius muscle inferolaterally. For more information on these muscles, see Applied Surgical Anatomy of the Thigh in Chapter 9 and Posterolateral Approach to the Tibia in Chapter 11.
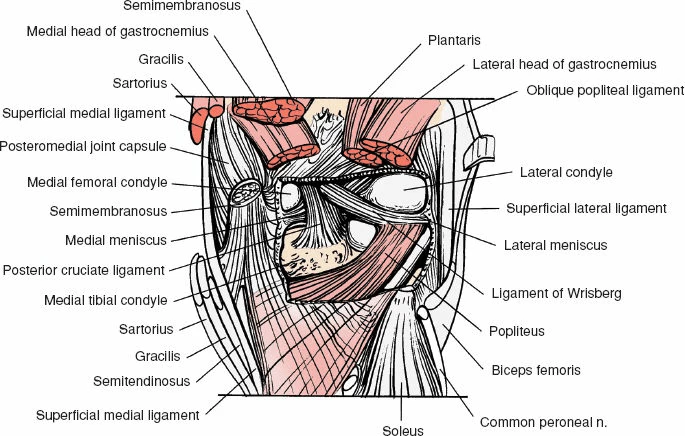
The floor of the popliteal fossa is formed by the popliteus, one of the few muscles in the body whose origin is distal to its insertion. The tendon enters the joint by passing through a gap in the posterolateral capsule, beneath the arcuate ligament.
Popliteus
Origin: Popliteal surface of tibia above soleal line.
Insertion: Lateral epicondyle of femur and posterior aspect of lateral meniscus.
Action: Rotates femur laterally on tibia.
Nerve supply: Tibial nerve.
The popliteus muscle unlocks the knee from its fully extended (screw home) position. It also draws the lateral femoral condyle backward on the tibia and pulls the lateral meniscus back, preventing it from being trapped between the tibia and femur. The convex rounded posterior aspect of the lateral tibial plateau allows this movement to take place.
Images: