Ankle FractureS Dislocations
Ankle FractureS Dislocations
key points (most commonly asked points) click on buttons below
Anatomy Mechanisms Radiographs Treatment
Lateral malleolus IS the Most commonly fractured
most commonly external rotation with the foot supinated
measure clear space 1 cm above joint normal <6 mm on both AP and mortise views .
posterior malleolar fracture with > 25% or > 2mm step-off IS an Operative indication .
anatomic reduction is considered most important factor for satisfactory outcome
Pre-reading Quiz: Use this quiz to test your background knowledge
1-A 32-year-old taxi driver sustains a twisting ankle injury An AP ankle radiograph is provided in Figure A.What are the diagnosis:
2)A 33-year-old male sustained a left ankle injury 1 month ago.The patient was originally seen in the emergency department of a local hospital, where the evaluating physician read his radiographs negative but his pain dose not improved associated with intermittent swelling.An AP ankle radiograph is provided in Figure A.What are the diagnosis?
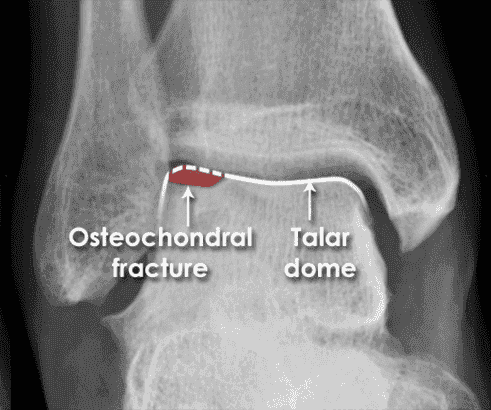 Osteochondral fractureLoss of the normal talar dome cortex contour due to an osteochondral fracture Osteochondral lesions of the talus are believed to occur after 2% to 6% of all ankle injuries. Patients with unexplained chronic ankle pain have been shown to have osteochondral lesions in 81% of cases. Treatment initially is non-operative with immobilization, anti-inflammatories and physical therapy. Nonoperative treatment has a reported success rate of 45% to 50%. Persistent symptoms are treated operatively with better results. Arthroscopic procedures with fragment excision and bone marrow stimulation has been shown to have a 87% success rate.
Osteochondral fractureLoss of the normal talar dome cortex contour due to an osteochondral fracture Osteochondral lesions of the talus are believed to occur after 2% to 6% of all ankle injuries. Patients with unexplained chronic ankle pain have been shown to have osteochondral lesions in 81% of cases. Treatment initially is non-operative with immobilization, anti-inflammatories and physical therapy. Nonoperative treatment has a reported success rate of 45% to 50%. Persistent symptoms are treated operatively with better results. Arthroscopic procedures with fragment excision and bone marrow stimulation has been shown to have a 87% success rate.
.
Facts
One of the most common skeletal injuries seen by physicians
Fractures of the malleoli are caused by rotational mechanisms, most commonly external rotation with the foot supinated
Incisura fibularis: groove along the distal lateral tibia in which the fibula lies
Lateral malleolus: lateral flare of the distal fibula Most commonly fractured
Inner surface divided by a groove that defines the anterior (larger) and posterior colliculus
Anterior colliculus is the attachment for the superficial deltoid ligament
Posterior colliculus is the attachment for the deep deltoid ligament
Posterior malleolus: posterior flare of the distal tibia Integrity important for posterior joint stability
Mortise: formed by the distal tibial articular surface (plafond), medial and lateral malleoli Articulates with the talar dome
Talar dome is wider anteriorly
In dorsiflexion, talar dome forces fibula laterally and into ER
In plantarflexion, the talar dome rotates internally due to checkrein action of the deltoid ligament
Normal ROM: dorsiflexion of 30° and plantarflexion of 45°
Minimum functional ROM: -10° to 20°
Axis of rotation is 20° externally rotated compared to knee
Leg has 4 compartments: scroll the image
Anterior: tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius, anterior tibial vessels and deep peroneal nerve
Lateral: peroneus longus, peroneus brevis and superficial peroneal nerve
Deep posterior: flexor digitorum longus, flexor hallucis longus, tibialis posterior, posterior tibial vessels and the tibial nerve
Superficial posterior: gastrocnemius, plantaris and soleus
Local structures:
Lateral: Peroneal tendons pass posterior to the lateral malleolus under the peroneal retinaculum
Superficial to the peroneals at this level is the sural nerve and lesser saphenous vein
Medial:
Posterior to the medial malleolus lie the tibialis posterior, flexor digitorum longus and flexor hallucis longus tendons, the posterior tibial vessels and tibial nerve These structures pass under the laciniate ligament (medial malleolus to calcaneus)Anterior to the medial malleolus are the saphenous vein/nerve
Anterior:
Under the extensor retinaculum (anteromedial tibia to anterolaterlal fibula) lie the tibialis anterior, extensor hallucis longus, extensor digitorum longus and peroneus tertius tendons, the deep peroneal nerve and the anterior tibial vesselsSuperficial to the extensor retinaculum is the superficial peroneal nerve
Posterior:
Achilles and plantaris tendons
Ligaments:
Medial ligament complex: deltoid ligament is the primary stabilizer of the ankle, resists valgus stress and lateral translation of the talus
Originates from medial malleolus
Superficial portion:
- originates from anterior colliculus and is comprised of 3 parts:
- Tibionavicular: attaches to navicular, suspends calcaneonavicular (spring) ligament
- Tibiocalcaneal: attaches at sustenaculum tali, prevents valgus
- Tibiotalar ligament: attaches along medial talar body
Deep portion:
primary medial stabilizer of the ankle, attaches to non-articular portion of medial talus
Intraarticular but extrasynovial
Disruption of the deltoid (or the medial maleollus) results in abnormal talar motion
Lateral ligament complex:
- originates from lateral malleolus, not as strong as medial
- Anterior talofibular ligament (ATFL): weakest, often first to fail
- Attaches at talar neck
- Prevents anterior subluxation of talus (anterior drawer)
- Posterior talofibular ligament (PTFL): strongest, often results in avulsion rather than rupture
- Attaches at lateral talar tubercle
- Prevents posterior subluxation of talus
Calcaneofibular ligament (CFL): stabilizes subtalar joint and resists inversion
- Attaches at superior lateral calcaneus
- Syndesmosis ligament complex: exists between the distal tibia and fibula at the level of the plafond
- Consists of the anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), transverse tibiofibular ligament (TTFL) and interosseous tibiofibular ligament (ITFL)
- Stabilizes the mortise, preventing migration of the talus
Presentation
- Patients typically present with ankle pain and variable amounts of swelling and ecchymosis
- Identify position of foot and direction of injury (e.g. inversion) when posible
- Evaluate entire leg for fibula fractures
- Ottawa ankle rules: radiographs are warranted when pain is present around malleoli and either:
- Tenderness to palpation of the posterior lateral malleolus (distal 6 cm)
- Tenderness to palpation of the posterior medial malleolus (distal 6 cm)
- Inabiltiy to take 4 steps immediately after injury and at presentation
- Isolated syndesmotic injury (high ankle sprain) can mimic regular ankle sprain (involving the lateral ligament complex):
- Tenderness to palpation of AITFL
- Squeeze test can be performed by compressing the tibia and fibula together 5 cm proximal to ankle
- Pain along the syndesmosis is considered positive
- External rotation test: ER of the ankle with knee flexed and ankle in neutral
- Pain at the AITFL or PITFL is considered positive
- Tenderness to palpation over the soft tissue anteromedial to medial malleolus may indicate deltoid injury
- Clinically evident ankle dislocations should be reduced immediately and then imaged
- Ankle dislocations without fracture are very rare
- Diabetic patients with low-energy injuries may have Charcot (neuropathic) arthropathy
- Assess NV status and identify associated injuries, particularly around the hindfoot, navicular and 5th MT
- Compartment syndrome: sustained increase in compartment pressure due to inflammation and edema in one or more of the leg compartments leading to vascular compromise and muscle death
- Muscle death occurs 6-8 hours after the onset of compartment syndrome
- Severe pain with passive motion of the toes/foot is often first sign
- Other signs include tense swelling of the calf, diminished pulses, pain out of proportion to injury and paresthesias
- Serial neurovascular exams are required as compartment syndrome can develop more than 24 hours after injury
- Compartment pressures should be measured in patients with clincal signs of compartment syndrome
- Compartment pressure > 30 mmHg or within 30 mmHg of the diastolic blood pressure warrant urgent fasciotomies of the leg compartments
- Deep posterior compartment pressure may be elevated in the presence of a soft superficial compartment
- Missed posterior compartment syndrome can result in claw toe deformity
Imaging
Radiographs
AP, lateral and mortise views of the ankle are standard examinations
AP:
Tibiofibular overlap: < 10 mm is abnormal and implies syndesmotic injury
Tibiofibular clear space: > 5 mm is abnormal and implies syndesmotic injury
Normal AP ankle
Lateral:
Identify posterior malleolus and anterior talar avulsion fractures
Talar dome should be centered and congruous under the tibial plafond
Normal lateral ankle
Mortise:
Taken with foot in 20° of IR
Medial clear space: > 4 mm is abnormal and indicates lateral talar shift (deltoid rupture)
Talar tilt: distal tibial articular surface should be parallel with superior talar articular surface
Difference of > 2° suggests talar tilt and ligamentous disruption
Talocrural angle: angle subtended by intermalleolar line (connecting distal-most points of both malleoli) and distal tibial articular surface should be between 8°-15°
A smaller angle indicates fibular shortening
Tibiofibular overlap: < 1 mm implies syndesmotic disruption
Normal ankle mortise
Stress view:
Performed by applying ER force to the ankle with foot dorsiflexed
Widening of the syndesmosis (decrease in tibiofibular overlap) indicates syndesmotic injury
Widening of the medial clear space indicates deltoid ligament injury
CT: may be indicated for complex fractures
Can detect impaction injuries to the plafond
Impaction of the anteriomedial or anteriolateral corners is a poor prognostic sign
MRI: can be used to evaluate subtle or stress fractures as well as ligament, capsule and tendon injuries
Classification
Lauge-Hansen: based on mechanism of injury, first word indicates position of foot during injury, second word indicates direction of deforming force
Each mechanism is an injury progression with each stage representing increasing severity
Injury begins in one location and proceeds around ankle depending on mechanism force
Supination-adduction =(webar A)
(10-20%): only type associated with medial talar displacement
Transverse/avulsion-type fibular fracture or a lateral ligament rupture
Vertical medial malleolar fracture
Supination-external rotation (40-75%)
ATFL disruption
Spiral fracture of distal fibula (posterosuperior to anteroinferior)
PTFL disruption or posterior malleolus fracture
Transverse/avulsion-type medial malleolus fracture or a deltoid ligament rupture
Pronation-abduction (5-20%)
Transverse/avulsion-type medial malleolus fracture or a deltoid ligament rupture
Syndesmotic ligament rupture or avulsion fracture
Short oblique distal fibular fracture at/above syndesmosis (lateral comminution/butterfly fragment common
Pronation-external rotation (5-20%)
Transverse/avulsion-type medial malleolus fracture or a deltoid ligament rupture
ATFL disruption
Spiral distal fibular fracture at/above syndesmosis (anterosuperior to posteroinferior)
PTFL disruption or avulsion
 Lauge-Hansen classification
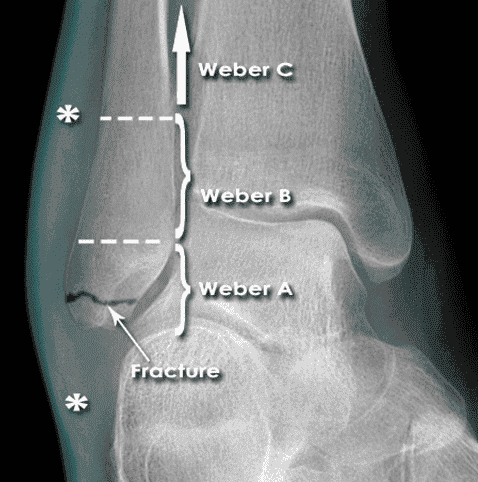
Danis-Weber: based on level of fibula fracture - the more proximal, the higher the risk of syndesmotic injury and instability
Type A: fracture below the level of the plafond
Associated with vertical or oblique fracture of the medial malleolus.
Corresponds to Lauge-Hansen SA
Type B: fracture at or near the level of the plafond
Most common ankle fracture
Often an obliqiue/spiral fracture caused by ER
50% associated with rupture of the anterior synesmosis
Corresponds to Lauge-Hansen SER
Type C: fracture above the level of the plafond
Results in syndesmotic disruption and commonly a medial injury
Includes Maisonneuve fractures (see below)
Corresponds to Lauge-Hansen PA and PER
OTA: tibia/fibula, malleolar segment (44)
Based primarily on fracture level in relation to syndesmosis
Type A: infrasyndesmosis
A1: isolated infrasyndesmosis lateral malleolus
A2: infrasyndesmosis lateral and associated medial malleolus injury
A3: infrasyndesmosis lateral and associated posteromedial tibial fracture
Type B: transsyndesmotic
B1: isolated transsyndesmotic lateral malleolus
B2: transsyndesmotic lateral and associated medial malleolus injury
B3: transsyndesmotic lateral with medial lesion and fracture of the posterolateral rim of the tibia
Type C: suprasyndesmotic
C1: simple diaphyseal fibula
C2: complex diaphyseal fibula with associated medial injury
C3: proximal fibular fracture with associated medial injury
Eponyms:
Maisonneuve: ER type injury to the ankle with associated fracture of the proximal third of the fibula
Most resemble Lauge-Hansen PER 3 with anterosuperior to posteroinferior fibula fracture
Fibular fracture itself typically does not need fixation but presence indicates energy associated with medial malleolus fracture was dissipated up through the syndesmosis and fibula
Should increase suspicion for syndesmosis instability
Tillaux-Chaput: syndesmosis injury associated with AITFL avulsion fracture of the tibia
LeForte-Wagstaffe: syndesmosis injury associated with AITFL avulsion fracture of the fibula
Associated with Lauge-Hansen SER fracture patterns
Treatment
Goal of treatment is to restore joint alignment and stability
Correct fibular length and rotation
Restore normal talar mechanics - even slight displacement increases contact force between tibia and talus
Syndesmotic injuries: diagnosed by avulsion fractures of the syndesmotic ligaments, talar shift or physical exam
Injuries without static instability (normal non-stress radiographs) but with mild dynamic instability (mild widening on stress view): short period of immobilization with NWB splint/cast followed by rehabilitation
Static instability or significant dynamic instability require operative fixation
Reduce fibula in the incisura fibularis
Place screw through fibula and tibia via lateral approach 2 cm above plafond and engage either 3 or 4 cortices with the foot in maximum dorsiflexion (to prevent over-tightening of the syndesmosis)
Controversy exists regarding size of screw and timing/necessity of removal
Acute treatment of all fractures/dislocations: cleanse and dress open wounds or skin abrasions
Dislocations should be reduced under conscious sedation or local block
With knee in flexion (reduce achilles tension) place hand around hindfoot apply traction and reverse deformity against countertraction on the tibia
Reduce displaced fractures and place in a short leg splint (posterior with stir-up) with ankle at 90°
Confirm alignment with post-reduction films
Nonoperative indications: nondisplaced/stable patterns with an intact syndesmosis, fractures with stable anatomic reduction, patient who cannot tolerate operative treatment
Transition from splint (see above) to SLC when swelling subsides
NWB immobilization generally for 6 weeks
SER II injuries can be WBAT due to mechanical stability
Close follow up to monitor displacement
Operative indications:
In general: failure to achieve adequate reduction, displaced/unstable fracture patterns with syndesmotic and/or deltoid injury, open fractures
Lateral malleolus
Weber A:
Isolated injuries typically do not require fixation and do well with early functional rehabilitation
Fixation should be considered for large fragments in the presence of a medial fracture
Weber B:
Presence of talar shift or medial malleolar fracture warrants fixation
Fractures without talar or medial fracture but signs of deltoid ligament injury (tenderness to palpation or positive stress test) require fixation
Weber C:
Require fixation due to inherent instability of the injury
Medial malleolus
Fixation is required when there is a syndesmotic injury, persistent talar displacement despite fibular fixation or medial instability (deltoid rupture)
Posterior malleolus
Fixation is required when there is > 2 mm of displacement, involvement > 25% of the articular surface or persistent subluxation of the talus posteriorly
Operative treatment:
If unable to treat patient acutely, allow patient and soft tissues to stabilize for up to 7 days before attempting ORIF
Elevate/ice ankle to reduce swelling
In situations of extreme soft tissue injury or expected prolonged delay of surgery, external fixation can maintain a provisional reduction
Lateral malleolus: in general, perform fibular fixation first through a direct lateral incision
Weber A: lag screw or tension band wiring
Weber B/C: posterior anti-glide plate or lag screw with lateral 1/3 semitubular neutralization plate
After fixation, intraoperative stressing of the syndesmosis complex to determine if syndesmosis fixation is required (see above)
Performed by applying ER force to the ankle with the foot dorsiflexed or lateral translation force to the fibula with a towel clip
Widening of the syndesmosis (decrease in tibiofibular overlap) under fluoroscopy indicates syndesmotic injury
In cases of deltoid rupture (medial clear space > 4 mm), the talus generally follows the fibula
Fixation of the fibula should restore the talar alignment and deltoid repair is not necessary given intact medial malleolus
Medial malleolus: through a direct medial incision
Generally fixed with two cancellous screws or a tension band construct
Posterior malleolus: usually reduces with reduction of the fibula
Can be fixed with one or two lag screws placed percutaneously anterior to posterior or with posterior anti-glide plate
Complications
Ankle stiffness: often due to prolonged immobilization
Compartment syndrome (~1%): urgent fasciotomies are required to release pressure and avoid muscle death
Infection: < 2% in closed injuries
Malunion: commonly a shortened/rotated fibula leading to pain or an elongated medial malleolus leading to instability
Nonunion: rare but is more commonly associated with a closed treated medial malleolus due to interposed soft tissue
Revision or excision may be required
Posttraumatic arthritis: a consequence of any articular injury, can be theoretically minimized with anatomic reduction
Reflex sympathetic dystrophy: rare, reduce risk with anatomic reduction and early return to motion
Wound problems: injuries undergoing operative fixation in the presence of abrasions or fracture blisters are at a 2x increased chance of wound complications