-DISEASE HISTORY")
Hip Dysplasia)-DISEASE HISTORY
Developmental Dislocation (Dysplasia) of the Hip (DDH)-DISEASE HISTORY
Prior to Its Recognition as a Disease
The disability of a dislocated hip has been mentioned for centuries, but understanding of the condition was poor. Hippocrates (460–357 BC)257 clearly described the disabling effects of a dislocation of the hip.
The British Museum has a specimen of a dysplastic hip from Neolithic times and a bronze figurine with congenital dislocation from Hellenistic times. Although the disability of infantile dislocated hip was very well known in the Medi- terranean world by the end of the first millennium BC, its etiology was poorly understood. In France, Andry mentioned the condition in
Hip dislocation was considered either accidental or spontaneous (symptomatic) until Guillaune Dupuytren (1777–1835) described a failure of fetal hip development and classified it as a third variety called “original or congenital dislocation. He considered the condition incurable.
Illustrations of a normal hip and a dislocated hip
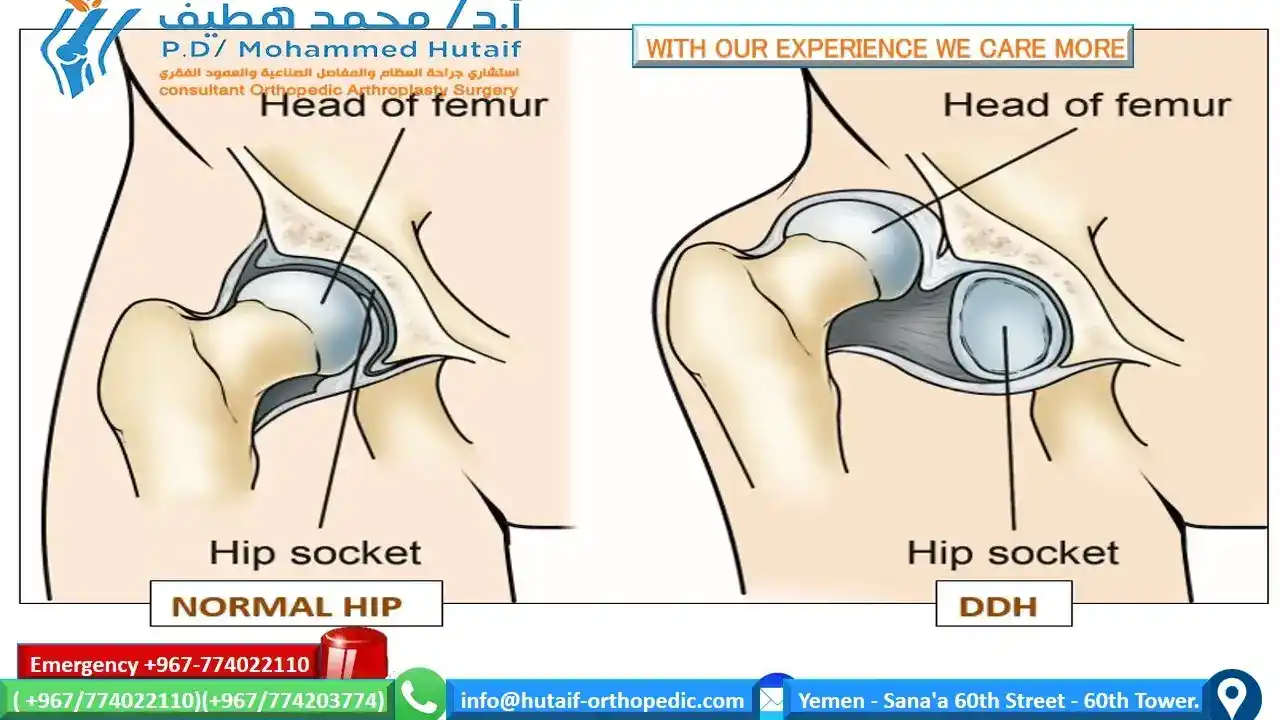
(Left) In a normal hip, the head of the femur fits firmly inside the hip socket. (Right) In severe cases of DDH, the thighbone is completely out of the hip socket (dislocated).
Recognition of DDH as a Disease
The first classical monograph about congenital hip dislocation was written by Charles Gabriel Pravaz of Lyon in 1837.
For treatment he recommended manipulation of the hip in extension and abduction, with pressure on the greater trochanter to bring the femoral head into the acetabulum. The reduction was maintained by prolonged traction. Paci (1887) and Adolf Lorenz described a forcible reduction by manipulation and cast ing (frog-leg position), which was later modified by Denuce (1898); however, complications of these treatments were common and severe.
At the turn of the twentieth century, the diagnosis of a congenital dislocated hip was usually made in older children of walking age: the reduction was by forceful manipulation, maintenance of reduction was by splinting the hip in abduction, and the results were frequently poor.
Medical attention was then directed toward more effective techniques of reducing dislocated hips in older children of walking age.
Lange developed a method of traction on the extended thigh and application of hip flexion and abduction to obtain the reduction.
The reduction was then maintained by casting. Putti recognized the problems of forceful reductions in older children and emphasized the importance of early diagnosis and treatment. He even suggested the necessity of beginning treatment at the moment the deformity was observed, even on the day of birth.
Most of the classic historical articles address treatment of the persistently dislocated hip, but few had satisfactory outcomes. Craig introduced an overhead traction technique to reduce the hip into the acetabulum; the reduction was held by a cast or splint.
In 1964, Hoffmann-Daimler developed a flexible bandage in which the hip was flexed and abducted at a slow pace and the reduction was accomplished in 8 to 14 days.
Hanausek developed an apparatus with a metallic base plate and movable thigh supports, which were adjusted to achieve the reduction.
Kramer used traction and developed pathways of hip reduction by gradual flexion and abduction of the hip.
Fettweis developed a technique of hip reduction using a squatting-position cast. These techniques often required prolonged hospitalization and had a significant rate of complication.
Gradually the knowledge developed that diagnosis at an early age and gentle reduction were necessary for success.
IN This Artical
next page: