Hip Dysplasia-Symptoms-Doctor Examination-DIFFERENTIAL DIAGNOSIS
Developmental Dislocation (Dysplasia) of the Hip (DDH)-Symptoms-Doctor Examination-DIFFERENTIAL DIAGNOSIS
Some babies born with a dislocated hip will show no outward signs.
PATIENT HISTORY AND PHYSICAL FINDINGS
■ Hip dysplasia can be diagnosed clinically in newborns and young infants owing to instability of the hip.
■ Patients with a history of hip dysplasia are typically followed radiographically until adulthood to ensure normal acetabular development.
■ Older children without a prior history of developmental hip dysplasia are typically diagnosed with radiographs based on clinical suspicion, especially when significant risk factors are present.
■ Risk factors include breech position, female, first-born, and oligohydramnios. Developmental hip dysplasia is associated with other “packaging disorders.”
■ Patients sometimes present in childhood with a limp, hip pain, limb-length discrepancy, or asymmetric hip abduction, particularly those with underlying neuromuscular conditions.
■ Routine screening for hip dysplasia in neuromuscular conditions with radiographs is widely performed.
■ Examinations and tests to perform include:
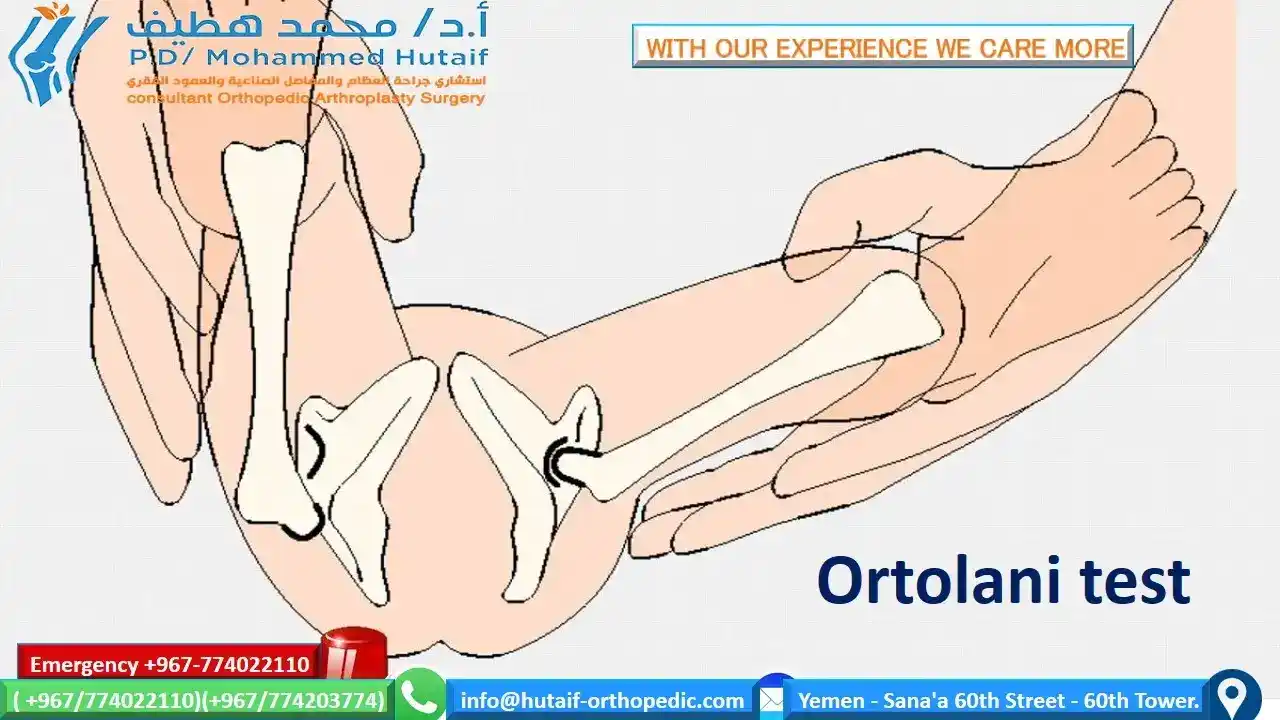
■ Ortolani test: Positive if a clunk is felt as a dislocated hip reduces.
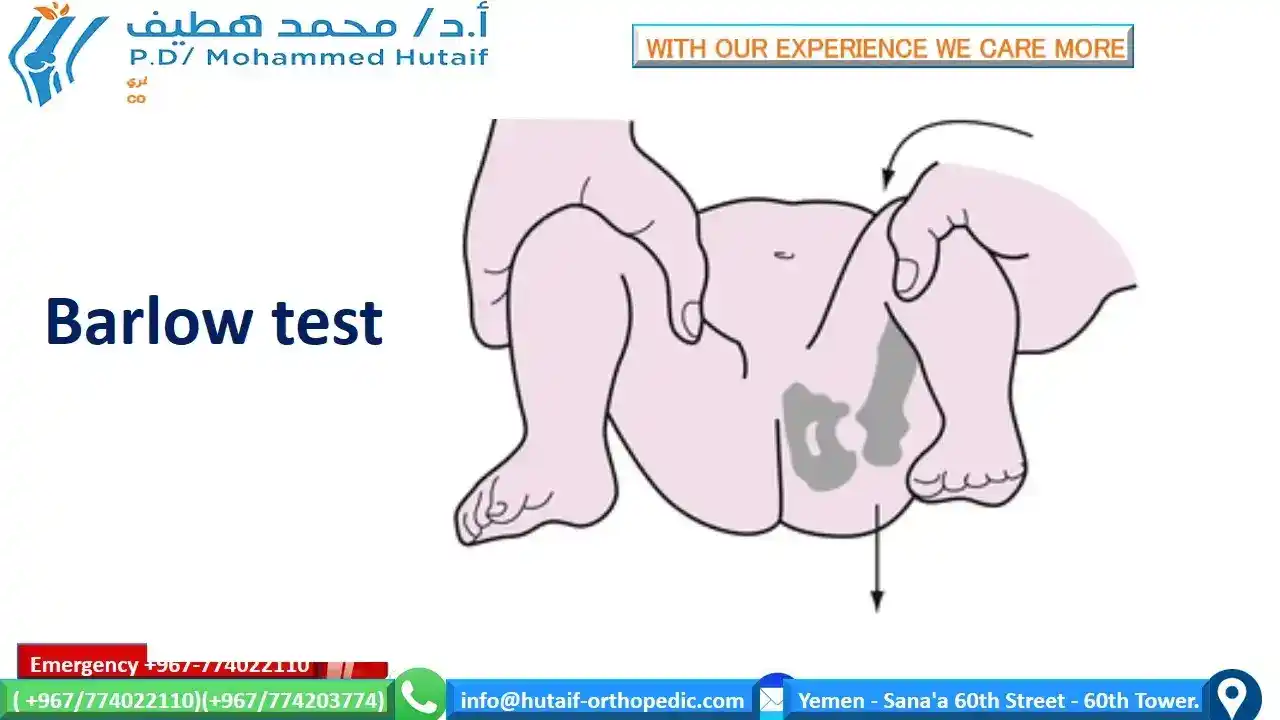
■ Barlow test: Positive if a clunk is felt as a reduced hip dislocates.
■ Hip abduction: In a normal hip, abduction should be more than 60 degrees and symmetric. This may be the only abnormal sign in infants. A difference of 10 degrees or more is significant.
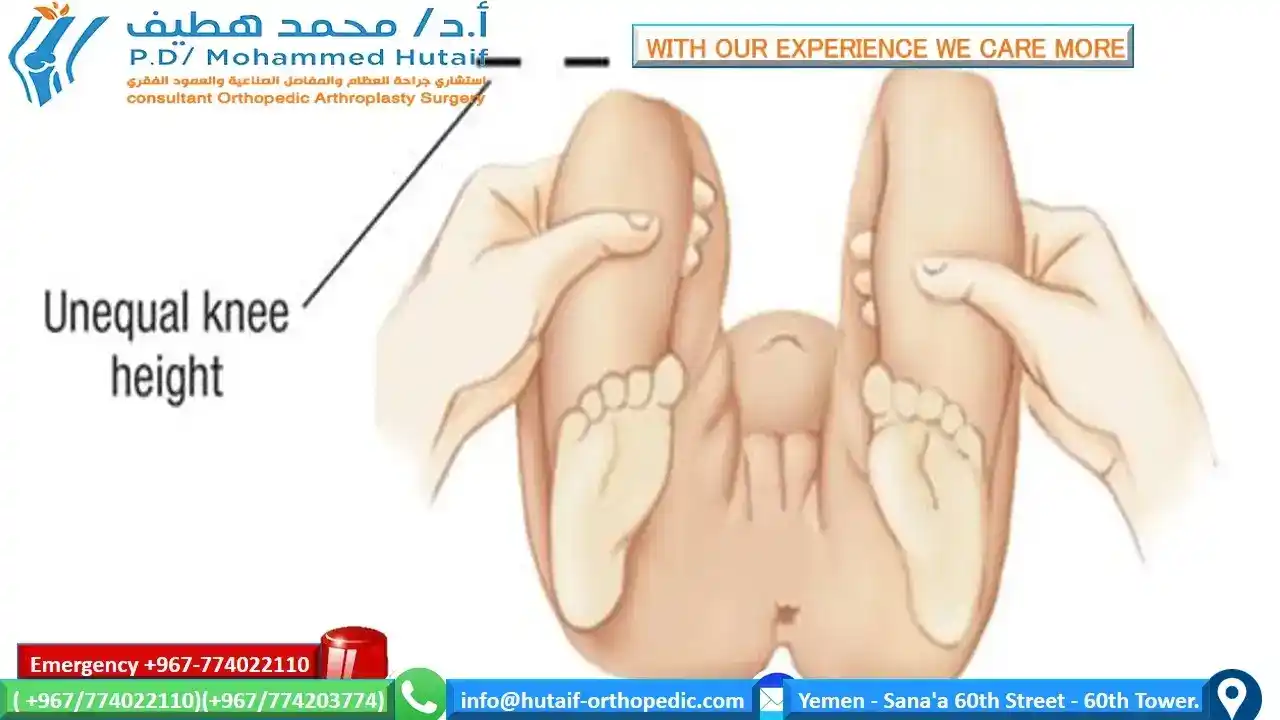
■ Galeazzi sign: A difference in thigh length is a positive result. A positive Galeazzi sign can indicate a dislocated hip, a short femur, or a congenital hip deformity.
■ Abnormal skin folds can occur in normal children but may also indicate asymmetric hip abduction.
■ Limp with ambulation, Trendelenburg sign, or limp associated with limb-length discrepancy may be the only abnormal sign in older children.
Contact your pediatrician if your baby has:
- Legs of different lengths
- Uneven skin folds on the thigh
- Less mobility or flexibility on one side
- Limping, toe walking, or a waddling gait
Doctor Examination
In addition to visual clues, your child's doctor will perform a careful physical examination to check for DDH, such as listening and feeling for "clunks" as the hip is put in different positions. The doctor will use specific maneuvers to determine if the hip can be dislocated and/or put back into proper position.
DDH examination
During the exam, your child's doctor will maneuver your baby’s legs and hips in certain ways to detect hip instability.
Newborns identified as at higher risk for DDH are often tested using ultrasound, which can create images of the hip bones. For older infants and children, X-rays of the hip may be taken to provide detailed pictures of the hip joint.
DIFFERENTIAL DIAGNOSIS
■ Slipped capital femoral epiphysis
■ Legg-Calvé-Perthes disease
■ Congenital coxa vara
■ Proximal femoral focal deficiency
IN This Artical
next page: